Fig. 28.1
Typical appearance of a uterus didelphus with the septum running from the bladder cephalad to the Douglas. Dividing the Douglas cavity up to the anterior wall of the rectum

Fig. 28.2
The operation starts by dividing the septum anteriorly bur as extensive as possible posteriorly as to make a unique cavity of Douglas
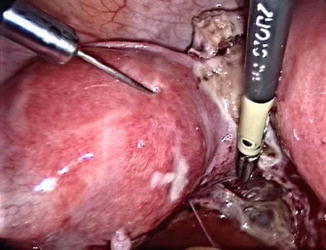
Fig. 28.3
The walls are infiltrated on the medial side with Ornitocine diluted 1:200 using a laparoscopic needle armed with a Luer lock syringe of 50 ml
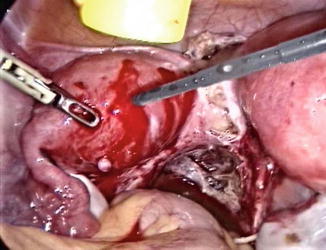
Fig. 28.4
A Manhez needle (Karl Storz Gmbh & Co Tuttlingen Germany) is used to delineate the first incision in the superficial layers of the myometrium
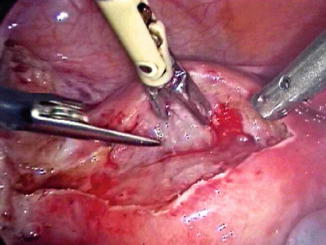
Fig. 28.5
For the deeper layers of the myometrium and for opening the endometrial cavity scissors are used to reduce the thermal spread on the tissues to zero by only using the crush effect of the scissors. Short burst of bipolar electrical energy, delivered through a Robi fenestrated forceps (Karl Storz Gmbh & Co Tuttlingen Germany), are used to clear the vision of the surgeon whilst lavage and aspiration are performed to clear the surgical field of blood
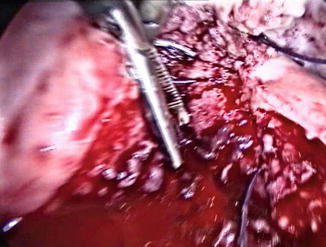
Fig. 28.6
The deeper muscle layers, to close the endometrial cavity, are united by Polyglactin 0 (Vicryl Ethicon)
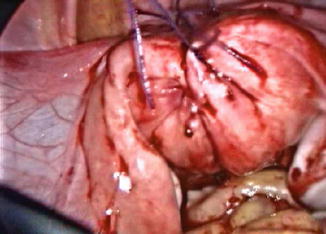
Fig. 28.7
The superficial muscle layer at the level of the serosa are closed by a hemostatic inverted suture of Polyglactin 1 according to the technique of Michel Degueldre
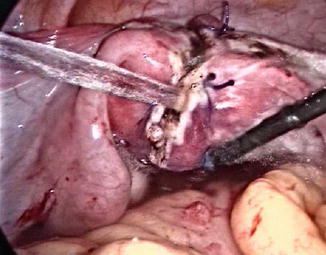
Fig. 28.8
At the end of the procedure Icodextrin 4 % (Adept Baxter healthcare SA) is used to float the uterus in the small pelvis as to minimise adhesion formation
Step 1: Establishment of Laparoscopy
A 20 cm Veress needle is inserted through an 1 cm incision as deep as possible in the umbilicus. The abdominal wall is elevated so that the needle penetrates perpendicular the fascia and the peritoneum. A pneumoperitoneum of 20 mmHg is installed. The CO2 gas is brought through a water bottle at 37 °C and is heated 20 cm from its entry into the abdomen. Allowing the gas to pass from 32 °C at the wall inlet to be heated up to 35 °C at its entry in the abdominal cavity. The humidity reaches up to 95 %. A pyramidal trocar of 12 mm is introduced after enlarging the umbilical incision and is brought into contact with the fascia. The fascia is hooked and the trocar is pushed into the abdominal cavity at an angle of 45° or less with the pressure of the bodyweight, the dominant hand guiding the trocar in the direction of the small pelvis. The non-dominant hand is wrapped around the trocar and has a brake function. This maneuver is comparable with the direct entry method. The intra-abdominal pressure is reduced to 16 mmHg. The patient is tilted into maximal Trendelenburg to let the bowels slip into the upper abdomen. The Trendelenburg is reduced to 15° and the operation is started.
Step 2: Opening of the Cavities
The two horns are brought into view. In most cases there is a septum between the two horns dividing the Douglas.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


