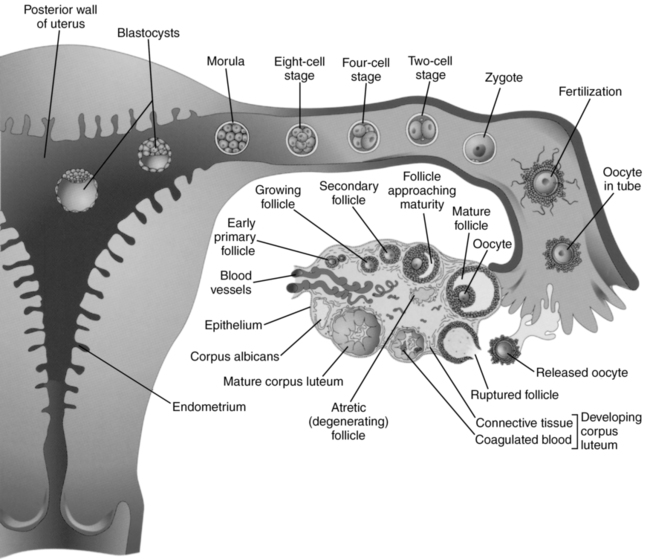
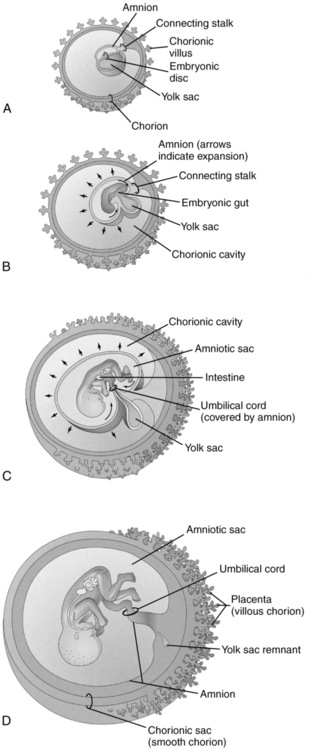
CHAPTER 23 first-trimester pregnancy loss. extraembryonic membrane that lines the chorion and contains the fetus and amniotic fluid. consists of an outer trophoblast and an inner cell mass. fetal heart rate below 90 beats per minute. name applied to the endometrium during pregnancy. portion of the endometrium on which the implanted conceptus rests. decidua that covers the surface of the implanted conceptus. decidua exclusive of the area occupied by the implanted conceptus; aka decidua vera. term used for a developing zygote through the tenth week of gestation. length of time based from conception. gestational weeks 6 through 10. visualization of the amniotic cavity without the presence of an embryo. length of time calculated from the first day of the last menstrual period. fluid-filled structure normally found in the uterus, containing the pregnancy. pregnancy located within the uterus. solid mass of cells formed by cleavage of a fertilized ovum. refers to the number of live births. centrally located endometrial fluid collection demonstrated with a coexisting ectopic pregnancy. fetal heart rate exceeding 170 beats per minute. provides nutrients to the embryo and is the initial site of alpha-fetoprotein. • Fertilization to implantation—approximately 5 to 7 days. • Ovum and sperm join in the distal fallopian tube, forming a zygote. • Cells of the zygote multiply, forming a cluster termed the morula. • Fluid rapidly enters the morula, forming a blastocyst. • After implantation—trophoblastic growth continues. • Maternal vessels erode, establishing a circulation on the maternal side of the forming placenta (chorion basalis). • Trophoblastic tissue covers the entire embryo, developing into the fetal side of the forming placenta (chorion frondosum). • Human chorionic gonadotropin (hCG) is secreted by the trophoblastic tissue. • Organogenesis is generally completed by the tenth gestational week. • Chorionic villi evenly surround the blastocyst. • Embryo is located between the amnion and yolk sac (Fig. 23-2, A). • Embryo folds into the amnion. • Amnion attaches to the anterior portion of the embryo. • Yolk sac becomes “pinched” near the embryo, forming the body stalk. • Chorionic villi become more prolific near the implantation site (Fig. 23-2, B). • Amnion begins to fill more of the chorionic cavity. • Yolk sac is pushed into the chorionic cavity. • Umbilical cord begins to develop about the seventh to eighth gestational week. • Areas of the chorion away from the implantation site become smooth (Fig. 23-2, C). • Amnion fuses to the smooth chorion. • Embryo or fetus lies within the amniotic cavity. • Chorionic villi and decidua basalis have formed a placenta (Fig. 23-2, D). • Produced by the trophoblastic cells of the developing chorionic villi. • Normally doubles every 30 to 48 hours during the first 6 weeks of pregnancy. • Peaks at the tenth gestational week (100,000 mIU/mL). • Declines after the tenth week and levels out at about 18 weeks (5000 mIU/mL). • Gestational sac should be identified transvaginally after the hCG levels reach 1000 mIU/mL and as early as 500 mIU/mL. • Establishes gestational age before visualization of an embryonic disc. • Measures the length, height, and width of the inner-to-inner borders of the gestational sac. • First-trimester screening for chromosomal abnormalities. • The gestation should be 11 weeks, 0 days, to 13 weeks, 6 days, and the crown–rump length (CRL) should be a minimum of 45 mm and a maximum of 84 mm. • Midsagittal section of the fetus should be in a neutral spine-down position. • Magnify so that only the fetal head and upper thorax should be included in the image. • Maximum thickness of the subcutaneous translucency between the skin and soft tissue overlying the cervical spine is measured. • Calipers are placed on the hyperechoic lines, not in the nuchal fluid, from the inner-to-inner borders perpendicular to the fetus. • More than one measurement must be taken, and the maximum one is to be recorded. • Nuchal translucency exceeding 3 mm is abnormal. • Pitfalls include poor fetal position, maternal obesity, and mistaking the amnion for the fetal skin line. Sonographic Findings in the First Trimester
Assessment of the first trimester
Early embryology (fig. 23-1)
Blastocyst development (fig. 23-2)
Anatomy
STRUCTURE
DESCRIPTION
NORMAL SONOGRAPHIC FINDINGS
Abdominal wall
Physiological herniation of the fetal bowel into the umbilical cord
Bowel returns into abdomen, and herniation resolves by the eleventh gestational wk
Umbilical herniation contiguous with the umbilical cord
Abnormal if persists after 12 wks’ gestation
Cardiovascular system
First system to function in the embryo
Four heart chambers are formed by the eighth gestational wk
Cardiac motion as early as 5.5 wks
Cranium
Prosencephalon—forebrain
Mesencephalon—midbrain
Rhombencephalon—hindbrain
Prominent cystic space in the posterior portion of the brain (rhombencephalon)
Skeletal system
Vertebral bodies and ribs are forming at 6 wks
Arms and legs are forming at 7 wks
Ossification of the vertebral bodies and rib cartilage at 9 wks
Long bones form during the tenth wk
Spine appears as parallel echogenic linear structures in the center of the embryo or fetus
Long bones appear as hyperechoic linear structure(s) within the soft tissue of the extremities
Laboratory values
Human chorionic gonadotropin (HCG)
First-trimester measurements
Mean sac diameter (MSD)

Nuchal translucency
Indications for sonographic evaluation
GESTATIONAL FINDING
DESCRIPTION
NORMAL SONOGRAPHIC FINDINGS
ABNORMAL SONOGRAPHIC FINDINGS
Gestational sac (GS)
Fluid-filled structure normally found in the uterus, containing the developing embryo
First definitive sonographic finding to suggest early pregnancy
Anechoic structure represents the chorionic cavity
Echogenic rim represents decidual tissue and the developing chorionic villi
Beta hCG of 1000 mIU/mL should demonstrate a GS transvaginally
Round anechoic structure
Surrounded by a thick hyperechoic rim (2 mm)
Located in the mid- to upper portion of the uterus
Eccentric location within the endometrium
Transabdominal
5 mm mean sac diameter (MSD) about 5-6 wks
Double decidual sign evident with an MSD of 10 mm
Transvaginal
2-3 mm about 4-5 wks
Irregular or distorted GS
Large GS without evidence of YS
Abnormal uterine location
Visualization of amnion without concomitant embryo
Transabdominal
Failure to identify a YS with an MSD ≥20 mm
Failure to identify an embryo with cardiac activity in a GS ≥25 mm
Transvaginal
Failure to identify a YS with an MSD ≥8 mm
Failure to identify an embryo with cardiac activity in a GS ≥16 mm
Yolk sac (YS)
Located in the chorionic cavity
Provides nutrition to the embryo
Earliest structure visualized in the gestational sac
Attached to the embryo by the vitelline duct
Used as a landmark to locate the embryonic disc and early cardiac activity
Ultimately detaches from the embryo and remains within the chorionic cavity
Hyperechoic ring within the gestational sac
Round or oval in shape
Inner-to-inner border diameter should not exceed 6 mm
Transabdominal
Evident within an MSD of 20 mm
Transvaginal
Evident within an MSD of 8 mm
YS diameter exceeding 8 mm
Transabdominal
Failure to identify a YS with an MSD ≥20 mm
Failure to identify an embryo with cardiac activity in a GS ≥25 mm
Transvaginal
Failure to identify a YS with an MSD ≥8 mm
Embryo
Embryonic period extends from the sixth through the tenth gestational wks
Initially a local thickening adjacent to the yolk sac
Echogenic focus adjacent to the yolk sac
Transabdominal
Usually detected within an MSD ≥25 mm
Transvaginal
Usually detected in an MSD of ≥16 mm
Embryo too small for gestational sac
Transabdominal
Failure to identify an embryo with cardiac activity in a GS ≥25 mm
Transvaginal
Failure to identify an embryo with cardiac activity in a GS ≥16 mm
Amnion
Initially surrounds the newly formed amniotic cavity
Attaches to the embryo at the umbilical cord insertion
Expands with accumulation of amniotic fluid and growth of the embryo
Obliterates the chorionic cavity by the sixteenth wk
Thin hyperechoic line between the embryo and the yolk sac (chorion)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access