Ascites
Karen Y. Oh, MD
DIFFERENTIAL DIAGNOSIS
Common
Pseudoascites (Mimic)
Hydrops
Bladder Rupture
Bowel Perforation
Infection
Less Common
Tachyarrhythmia
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Pseudoascites (Mimic)
Abdominal wall musculature can mimic ascites
Surrounds the anterolateral liver margin but not seen posteriorly
More prominent with slightly oblique scan angle
True ascites is seen in other parts of abdomen, outlines organs
Hydrops
Fluid in 2 body spaces
Skin edema, pleural effusion, ascites, pericardial effusion
Nonimmune or immune hydrops
Polyhydramnios and placentomegaly also commonly present
Bladder Rupture
Initial ultrasound may show markedly enlarged bladder
Look for evidence of posterior urethral valves or urethral atresia
Less commonly due to prune belly or megacystis-microcolon
Bladder rupture results in urinary ascites
Thick-appearing bladder wall after decompression
Follow all fetuses with large bladder
Likely transient finding if otherwise normal urinary tract
Bowel Perforation
Initial ultrasound may show dilated bowel
Underlying atresia(s), volvulus, intussusception, meconium ileus
Often perforation event is occult, with ascites being the only finding
Look for signs of meconium peritonitis to confirm diagnosis
Intraperitoneal calcifications
Meconium pseudocyst
Infection
Ascites may be isolated, but more commonly, is part of generalized hydrops
Look for hepatic or cerebral calcifications
Correlate with clinical history for maternal signs of infection or exposures
Helpful Clues for Less Common Diagnoses
Tachyarrhythmia
Sustained heart rate > 180-200 bpm
Ascites may be isolated and first sign of impending failure/hydrops
Always check heart rate in setting of isolated ascites
Image Gallery
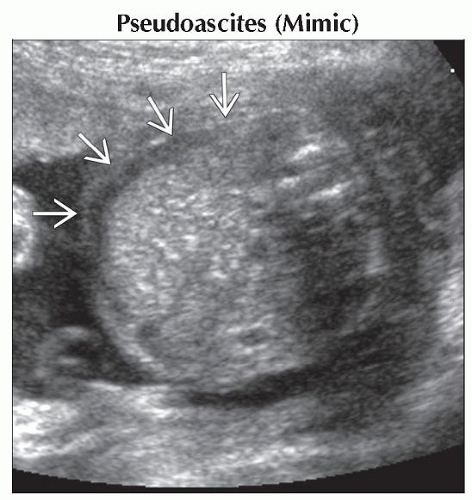 Axial oblique ultrasound shows a prominent hypoechoic linear area
 , lateral to the liver, which represents abdominal wall musculature and not ascites. This was not seen in other scan planes. , lateral to the liver, which represents abdominal wall musculature and not ascites. This was not seen in other scan planes.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|