Appendicitis
Appendicitis is one of the most common surgical emergencies in children. Over 70,000 cases are seen in the USA each year.1,2 The lifetime risk of appendicitis is 9% in boys and 7% in girls. Unfortunately, there is a lack of general consensus regarding its diagnosis and management.3
Pathophysiology
The spectrum of appendicitis ranges from simple inflammation to gross perforation. This concept was initially described by van Zwalenberg in 1905 and confirmed in an experimental model by Wangensteen in 1939.4,5 Obstruction of the lumen can occur from multiple causes including fecal material (fecalith), lymphoid hyperplasia, foreign body, or parasites. Fecaliths are present in roughly 20% of children with acute appendicitis and 30–40% of children with perforated appendicitis.6,7 Fecaliths and appendicitis are more common in developed countries with low-fiber diets compared to developing countries with high-fiber diets.8 Hyperplasia of the lymphoid tissue near the base of the appendix is also a common cause of appendiceal obstruction in children. Interestingly, the incidence of appendicitis closely resembles the amount of appendiceal lymphoid follicles present.9 Organisms such as Yersenia, Salmonella, and Shigella can cause a local or generalized reaction of the lymphoid tissue leading to obstruction. In similar fashion, parasitic infestations from Entamoeba, Strongyloides, Enterobius, Schistosoma, or Ascaris species and viral infections such as mumps virus, coxsackie virus B, cytomegalovirus, and adenovirus can lead to luminal obstruction secondary to lymphoid hyperplasia.10–18 In children with cystic fibrosis, obstruction may be due to abnormal production of mucus leading to painful distention with or without inflammation.19 Appendicitis in neonates is rare and warrants evaluation for cystic fibrosis and Hirschsprung disease.20 It is difficult to distinguish neonatal appendicitis from necrotizing enterocolitis confined to the appendix.21
Following obstruction, the appendix becomes distended from the accumulation of mucus and proliferation of bacteria. As intraluminal pressure increases, lymphatic and venous drainage are impaired resulting in local edema. A further increase in pressure will limit arterial inflow, thus jeopardizing tissue integrity and ultimately leading to tissue necrosis and perforation. Although the natural history of untreated appendicitis is usually perforation and abscess, not all patients will progress in this fashion. Resolution of untreated appendicitis has been described and may be the mechanism behind the clinical phenomenon of relapsing or chronic appendicitis.22,23
Historically, appendicitis has been considered a somewhat time-sensitive condition such that a significant delay in treatment may lead to an increased risk of perforation. It is for this reason that young children have a higher appendiceal perforation rate compared to older children.24 Younger children have less ability to understand or articulate their developing symptoms. As a result, perforation rates have been reported to be as high as 82% in children younger than 5 years and nearly 100% in 1-year olds.25
Age is not the only factor accounting for delays in treatment and therefore higher perforation rates. One of the biggest concerns contributing to this delay is the lack of access to health care. It follows that patients with poor access to health care will have higher perforation rates. Indeed, children with no insurance or public insurance have higher rates of appendiceal perforation compared to children with private insurance.26–29 Minorities also have higher perforation rates compared to whites.26–29 Encouragingly, settings in which patients have equal access to health care or a well-established primary care network eliminate these racial, ethnic, and socioeconomic differences.30,31
Clinical Presentation
Fever, tachycardia, and leukocytosis develop as a consequence of systemic inflammatory mediators released by ischemic tissues, white blood cells, and bacteria. The inflamed appendix then irritates the overlying peritoneum, typically by direct contact. This leads to focal peritonitis and localized right lower quadrant pain. This process explains the typical migrating pain from the umbilicus to the right lower quadrant. Any movement of the peritoneum will lead to an exacerbation of the pain. Thus, children will often demonstrate voluntary guarding of the right lower quadrant during the exam. Furthermore, children will usually resist walking and jumping due to the increased pain associated with such movement.
Laboratory studies often show a mild leukocytosis. A markedly elevated leukocyte count suggests perforation or another diagnosis. Patients with appendicitis will have higher leukocyte counts compared to patients without appendicitis.32 However a broad range of sensitivity (52–96%) exists, which limits the usefulness of this laboratory value alone. A left-shifted differential count may be a better diagnostic indicator, but a wide range in sensitivity (39–96%) also can lead to misinterpretation.33–35 Other inflammatory markers including C-reactive protein (CRP), procalcitonin, and D-lactate have also been investigated. Of these markers, only CRP has been shown to be useful. A value greater than 3 mg/dL has been associated with the definitive diagnosis of appendicitis when compared to children with abdominal pain from a different etiology.32 The combination of elevated leukocyte count and CRP level has the highest correlation of definitively diagnosing appendicitis.32,36 Although normal values of both leukocyte count and CRP make the diagnosis of appendicitis less likely, the clinical signs and symptoms should be carefully considered as appendicitis cannot be excluded based on normal laboratory values. A urine analysis is typically obtained and is usually free of bacteria, but a few or moderate number of red or white blood cells may be found as the inflammatory process of the appendix may locally affect the bladder or ureter.
The typical presentation of appendicitis as described previously is found in roughly 50% of patients.37 Children with appendicitis often present with wide deviations from this classic picture making for a challenging diagnosis. In patients with an atypical presentation of appendicitis, clinical scoring systems have been used to aid in making the diagnosis.38,39 Accuracy of these scoring systems has been inconsistent which limits their usefulness over clinical judgment.40–42 They have, however been shown to decrease the use of computed tomography (CT) scans.43 Recent studies have stratified patients into risk categories based on history, physical examination, and laboratory studies to determine which patients should have surgical consultation (high risk), additional imaging studies (medium risk), or be discharged (low risk).38–42 This is the most applicable use of a scoring system or clinical pathway at the present time.
Imaging Studies
Misdiagnosing appendicitis can lead to significant delays in treatment. Children are often diagnosed with gastroenteritis and parents are reassured that their child will improve, which may delay them from seeking further care. Epidemiologic data have shown the risk of a missed diagnosis in children to be higher in hospitals with a volume of less than one pediatric appendectomy per week.44 Historically, negative appendectomy rates of 10% to 20% were not only considered appropriate but advisable to minimize the number of patients with a missed diagnosis and to decrease perforation rates. Some authors have questioned this philosophy, citing the risk and expense of an avoidable operation.45 Appropriate use of diagnostic imaging can minimize both the negative appendectomy and perforation rates. Currently, the negative appendectomy rate from high-volume children’s hospitals is 3–4%.46–48 Despite the increased use of imaging studies, correctly diagnosing children less than 5 years of age continues to be challenging with negative appendectomy rates ranging from 13–17%.48
Ultrasonography (US) offers the advantages of being an efficient bedside technique that is noninvasive, requires no contrast, and emits no radiation. Thus, ultrasound should be the first imaging study utilized in patients with atypical presentations of appendicitis. Common ultrasound findings include a fluid-filled, noncompressible appendix, a diameter greater than 6 mm (Fig. 42-1), appendicolith, periappendiceal or pericecal fluid, and increased periappendiceal echogenicity caused by inflammation.49,50 Most studies demonstrate a sensitivity greater than 85% and specificity greater than 90%.51,52 However, ultrasound is operator dependent and results of published studies may not be similar to results obtained in many clinical settings. Patient factors such as bowel gas pattern, obesity, and guarding or movement can affect the accuracy. False-positive results may be due to a large appendix or another tubular structure being mistaken for the appendix. When a normal appendix is identified, it is a reliable study to rule out appendicitis. Unfortunately, only 10–50% of children with normal appendices can be identified.52–54 When a normal appendix is not seen, there is still a risk of appendicitis despite an otherwise normal ultrasound study.55 Graded compression ultrasound places pressure on the transducer to displace bowel loops and identify the appendix. The pressure is felt adequate if the psoas muscle and the iliac vessels are identified, which assure the range of view is posterior to the appendix. Furthermore, data from a large series employing upward graded compression, posterior manual compression, left oblique lateral decubitus position, and a low frequency convex transducer demonstrated that nearly all appendices could be identified with over 98% accuracy for correctly diagnosing appendicitis.56 Contrast-enhanced power Doppler ultrasound imaging demonstrated similar accuracy in a small study.57

FIGURE 42-1 This longitudinal view of an ultrasound in a patient with acute appendicitis shows an enlarged appendix measuring 11 mm. in diameter.
When ultrasound is unable to exclude or confirm appendicitis, additional imaging or observation with serial examinations is warranted. In order to avoid hospitalization for observation, many physicians obtain a CT scan. The findings of an enlarged appendix (>6 mm), appendiceal wall thickening (>1 mm), periappendiceal fat stranding, and appendiceal wall enhancement are useful diagnostic criteria (Fig. 42-2).58,59 For the most part, the sensitivity and specificity of CT are around 95%.60–66 These values are significantly lower in diagnosing perforated appendicitis.67 The perceived improved diagnostic accuracy of CT has led to a dramatic increase in the number of CT scans performed in children even though there is not good evidence that supports its routine use for the diagnosis of appendicitis.68–71

FIGURE 42-2 These three CT scans show differing presentations for appendicitis. (A) The appendix (arrow) is enlarged and has a thickened wall. There are no inflammatory changes such as periappendiceal fat stranding seen on this study. (B) The appendix (arrow) is enlarged and there is free fluid and inflammatory changes medially indicating likely perforation. (C) The patient presented with a one week history of pain and the appendix has perforated with the development of two abscesses (asterisks). In addition, a fecalith is seen medially (dotted arrow). This patient was initially managed nonoperatively with drainage of the abscesses and intravenous antibiotics. She underwent laparoscopic interval appendectomy 10 weeks following the initial admission.
There are, however, several concerns with CT. Some protocols require a delay in the emergency department for contrast administration, and younger children may require sedation. Recently, the ease of rapid helical CT has led to an estimated 200% increase in pediatric CT scans, significantly increasing radiation exposure in young patients.72 This has become a growing concern because although no direct connection between CT scan and malignancy has been made, lifetime radiation exposure has been linked to an increased risk of malignancy.73 It has been estimated that a complete abdominal CT scan is equivalent to 25.7 months of natural background radiation exposure.74 Developing tissues are more sensitive to the effects of radiation as evidenced by an increased risk of radiation-induced malignancy in patients exposed at a younger age.73,75 The risk of a fatal radiation-induced malignancy is estimated at 0.18% for a 1-year-old child. In other words, one death due to malignancy would result from an abdominal CT scan done on 555 1-year-old patients, whereas about twice as many 15-year-olds would need to be scanned to equal that risk. Although this estimate seems significant, it represents only a 0.35% increase in overall risk compared to the risk of cancer mortality with natural background radiation.76 Use of a staged imaging protocol, performing CT scan only if ultrasound findings are equivocal, has shown a reduction in the number of CT scans performed and therefore overall radiation exposure without sacrificing diagnostic sensitivity and specificity.77 In addition, international guidelines on radiation protection have implemented the ALARA principle (as low as reasonably achievable), thus decreasing radiation exposure in children by 30-50%.72,75,77 Although the overall increase in risk may be miniscule, it is important to attempt to limit radiation exposure when evaluating children with acute appendicitis.
Magnetic resonance imaging (MRI) is an intriguing nonradiation alternative to CT and is extremely accurate in diagnosing appendicitis.78 The current version of this technology makes it impractical for widespread application, but future generations of scanners could allow it to be the preferred diagnostic imaging modality.
Differential Diagnosis
Acute appendicitis can mimic virtually any intra-abdominal process and should be high on the differential diagnosis in children with abdominal pain.79 Causes of acute right lower quadrant pain that are often indistinguishable from appendicitis include tubo-ovarian pathologic processes, Crohn disease, mesenteric adenitis, cecal diverticulitis, Meckel diverticulitis, constipation, viral gastroenteritis, and regional bacterial enteritis (Yersinia and Campylobacter in particular). Lower abdominal pain or vague nonfocal pain can result from a urinary tract infection, kidney stone, ureteropelvic junction obstruction, uterine pathologic process, right lower lobe pneumonia, sigmoid diverticulitis, cholecystitis, pancreatitis, gastroenteritis, vasculitis, bowel obstruction, and malignancy (lymphoma). The most common diagnosis made in the presence of missed appendicitis is reported to be gastroenteritis.80 Although many of these conditions may seem easily distinguishable, they each possess a spectrum of presentation that overlaps with appendicitis.
Treatment
The treatment of appendicitis begins with intravenous fluids and broad-spectrum antibiotics to provide coverage of enteric organisms. Management after initiating antimicrobial therapy depends on the severity of inflammation and the discussion must therefore be separated into uncomplicated (nonperforated) and complicated (perforated appendicitis). This distinction, however, is not always clear. Diagnostic imaging may help but cannot accurately diagnose perforation and many patients will not undergo preoperative imaging.61 Even intraoperative assessment showed high rates of discordance when compared to histologic evaluation of gangrenous and/or ruptured appendicitis.81 Surgeons polled with photographs showed extreme incongruence on which patients had perforation,82 and a survey of American Pediatric Surgical Association members revealed that most surgeons base their practice patterns on individual preferences.3 For this reason, the literature focusing on perforated appendicitis must be viewed with caution.
In reality, appendicitis presents as a spectrum of disease and it is important to distinguish which patients are at higher risk of complications. The data comparing outcomes of nonperforated versus perforated appendicitis is extensive, but most studies fail to use a strict definition of perforation. One prospective study showed that defining perforation as a visible hole in the appendix or a fecalith in the abdomen effectively identified those with greater risk of developing intra-abdominal abscesses (Fig. 42-3).83 In addition, outcomes in gangrenous appendicitis are similar to acute appendicitis and many patients may actually be over-treated.84 Thus, in the following discussion, the management of uncomplicated appendicitis will include acute, suppurative, and gangrenous appendicitis whereas complicated appendicitis will be synonymous with perforated appendicitis.
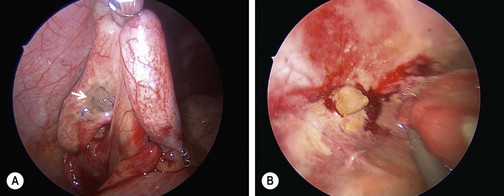
FIGURE 42-3 These two images depict the definition of perforation used in a prospective randomized trial.103 This definition of either (A) a hole in the appendix (arrow) or (B) stool in the abdomen was subsequently validated.83 An objective definition of perforation allows surgeons to compare outcomes data more accurately about perforated appendicitis.
Uncomplicated Appendicitis
After intravenous fluids and administration of broad-spectrum antibiotics, the current standard of care for uncomplicated appendicitis is appendectomy. Prophylactic antimicrobial agents should be given for 24 hours or less. In fact, a single preoperative dose of antibiotics has shown to decrease the risk of wound infection and abscess.85,86 Following appendectomy, patients are typically discharged within 24 hours. Additional postoperative antibiotics for acute appendicitis are not necessary or recommended.85,87 However, it may be reasonable to administer additional antibiotics for patients with suppurative or gangrenous appendicitis during the first 24 hours after appendectomy or longer based on the patient’s clinical status.
Recent data in adults suggests that administration of antibiotics without appendectomy may be sufficient to treat uncomplicated appendicitis. Multiple prospective randomized trials in adults have demonstrated similar outcomes from acute appendicitis treated with antibiotics alone with success rates ranging from 44% to 85%.88–92 Adults managed nonoperatively demonstrated fewer complications and less pain, although recurrence rates were high, ranging from 14% to 37%.93 There have been no prospective, randomized trials in children comparing antibiotics alone to appendectomy. Regardless of treatment modality, once antibiotics have been initiated, appendectomy is no longer considered to be an emergency and may even be considered somewhat elective.88,89,93–98 Until there is enough prospective randomized data in pediatric patients proving the efficacy of primary antibiotic treatment, appendectomy remains the standard of care for uncomplicated appendicitis. However, the need for operation may not be as urgent as previously thought.
Complicated Appendicitis
Patients with perforated appendicitis should receive postoperative antibiotics until clinical resolution has occurred. The antibiotic regimen employed for perforated appendicitis has traditionally been triple antibiotic therapy (ampicillin, gentamicin, and clindamycin or metronidazole). However recently there has been a shift towards more simple antibiotic regimens. Single agent therapy with piperacillin/tazobactam or cefotaxime, or double agent therapy with ceftriaxone and metronidazole, has been shown to be as efficacious as triple antibiotic therapy but is more cost effective.99–103 Several authors have highlighted a decrease in antibiotic expense with once daily dosing of ceftriaxone compared with multi-dose monotherapeutic agents. In addition, a prospective randomized study confirmed that single daily dosing of ceftriaxone and metronidazole is equal to and more cost effective than traditional triple antibiotic therapy in the treatment of perforated appendicitis.103 Therefore, current best evidence suggests once-a-day dosing with ceftriaxone at 50 mg/kg/day and metronidazole at 30 mg/kg/day provides the simplest and least expensive regimen.
Although the length of antibiotic course for perforated appendicitis is not yet standardized, current findings from multiple systematic reviews recommend continuation of antibiotics until resolution of clinical symptoms.85,102 This includes normalization of leukocyte count and differential, full return of gastrointestinal function, resolution of fever, and normalization of physical exam. In addition, if the duration of intravenous antibiotic therapy is less than 5 days, patients can be discharged safely on oral antibiotics to complete a 7-day course.104 A patient who is clinically well by postoperative day three is unlikely to develop an abscess.105 However, if a patient’s clinical symptoms have not resolved, it should raise the suspicion of an intra-abdominal abscess and intravenous antibiotics should be continued.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


