Chapter 104 Adolescent Development
See also Part XII and Chapters 555 and 556.
104.1 Adolescent Physical and Social Development
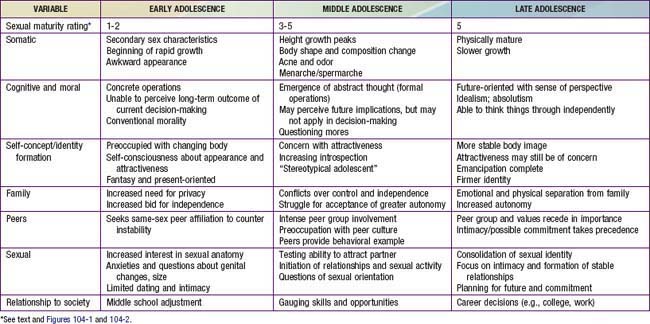
Young people undergo rapid changes in body structure and physiologic, psychological, and social functioning between the ages of approximately 9 to 10 and 20 yr. Adolescence consists of 3 distinct periods—early, middle, and late—each marked by a characteristic set of biologic, psychological, and social issues (Table 104-1). Hormones set this developmental agenda together with social structures designed to foster the transition from childhood to adulthood. Although individual variation is substantial, in both the timing of somatic changes and the quality of the experience, pubertal changes follow a predictable sequence. Gender and subculture profoundly affect the developmental course, as do physical and social stressors.
Early Adolescence
Biologic Development
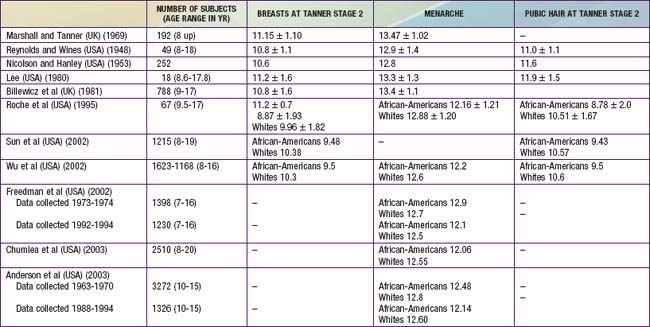
Data regarding the timing for the onset of puberty in girls are controversial (Table 104-2). Several studies from 1948 to 1981 identified the average age for the onset of breast development to range from 10.6-11.2 yr of age. Multiple reports since 1997 suggest a significantly earlier onset of breast development, ranging from 8.9-9.5 yr in African-American girls and 10.0-10.4 yr in white girls. There also appears to be a small secular trend toward decreasing ages for the onset of pubic hair development and menarche. The reasons for the larger decrease in age for breast development may include the epidemic of childhood obesity as well as exposure to estrogen-like toxins in the environment that include certain pesticides, plastics, phytoestrogens, and industrial compounds along with beef fattened with subcutaneous estrogen pellets.
It is less clear whether there is also a secular trend for decreasing age for onset of puberty in boys (Table 104-3). It appears that, over the past 40 yr, the average age for the onset of genital and pubic hair development may have decreased by about a year. The onset of puberty in African-American boys precedes that in white boys by at least 6 mo.

Once the onset of puberty has begun, the resulting sequence of somatic and physiologic changes gives rise to the sexual maturity rating (SMR), or Tanner stages. Figures 104-1 and 104-2 depict the somatic changes used in the SMR scale; Tables 104-4 and 104-5 also describe these changes. Figures 104-3 and 104-4 depict the typical sequence of pubertal changes in boys and girls, respectively. The range of normal progress through sexual maturation is wide.

Figure 104-1 Sexual maturity ratings (2 to 5) of pubic hair changes in adolescent boys (A) and girls (B) (see Tables 104-4 and 104-5).
(Courtesy of J.M. Tanner, MD, Institute of Child Health, Department for Growth and Development, University of London, London, England.)
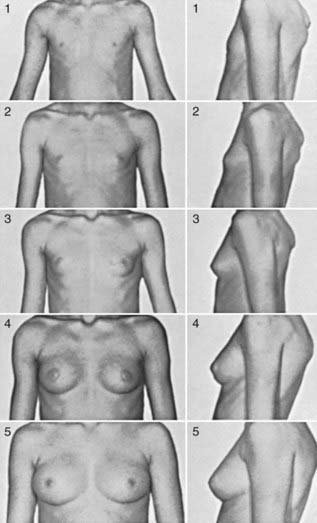
Figure 104-2 Sexual maturity ratings (1 to 5) of breast changes in adolescent girls.
(Courtesy of J.M. Tanner, MD, Institute of Child Health, Department for Growth and Development, University of London, London, England.)
Table 104-4 CLASSIFICATION OF SEXUAL MATURITY STATES IN GIRLS
| SMR STAGE | PUBIC HAIR | BREASTS |
|---|---|---|
| 1 | Preadolescent | Preadolescent |
| 2 | Sparse, lightly pigmented, straight, medial border of labia | Breast and papilla elevated as small mound; diameter of areola increased |
| 3 | Darker, beginning to curl, increased amount | Breast and areola enlarged, no contour separation |
| 4 | Coarse, curly, abundant, but less than in adult | Areola and papilla form secondary mound |
| 5 | Adult feminine triangle, spread to medial surface of thighs | Mature, nipple projects, areola part of general breast contour |
SMR, sexual maturity rating.
From Tanner JM: Growth at adolescence, ed 2, Oxford, England, 1962, Blackwell Scientific.
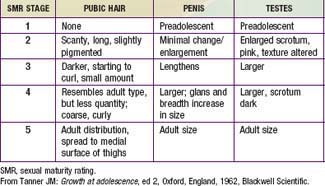
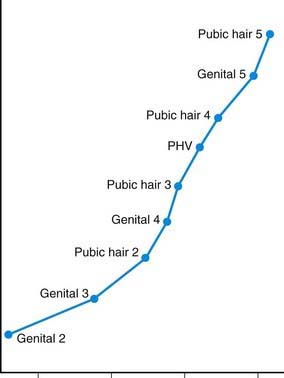
Figure 104-3 Sequence of pubertal events in males. PHV, peak height velocity.
(From Root AW: Endocrinology of puberty, J Pediatr 83:1, 1973.)
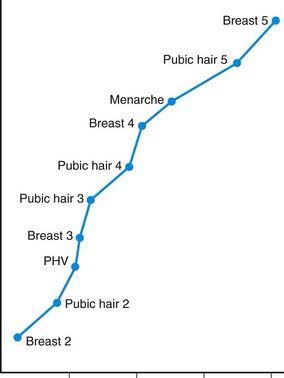
Figure 104-4 Sequence of pubertal events in females. PHV, peak height velocity.
(From Root AW: Endocrinology of puberty, J Pediatr 83:1, 1973.)
In girls, the 1st visible sign of puberty and the hallmark of SMR2 is the appearance of breast buds, between 8 and 12 yr of age. Menses typically begins 2- yr later, during SMR3-4 (median age, 12 yr; normal range, 9-16 yr) (see Fig. 104-4). Less obvious changes include enlargement of the ovaries, uterus, labia, and clitoris, and thickening of the endometrium and vaginal mucosa.
yr later, during SMR3-4 (median age, 12 yr; normal range, 9-16 yr) (see Fig. 104-4). Less obvious changes include enlargement of the ovaries, uterus, labia, and clitoris, and thickening of the endometrium and vaginal mucosa.
 yr. This is followed by penile growth during SMR3. Peak growth occurs when testis volumes reach approximately 9-10 cm3 during SMR4. Under the influence of LH and testosterone, the seminiferous tubules, epididymis, seminal vesicles, and prostate enlarge. The left testis normally is lower than the right. Some degree of breast hypertrophy, typically bilateral, occurs in 40-65% of boys during SMR2-3 due to a relative excess of estrogenic stimulation.
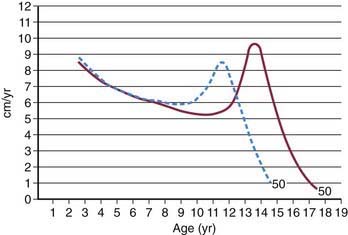
yr. This is followed by penile growth during SMR3. Peak growth occurs when testis volumes reach approximately 9-10 cm3 during SMR4. Under the influence of LH and testosterone, the seminiferous tubules, epididymis, seminal vesicles, and prostate enlarge. The left testis normally is lower than the right. Some degree of breast hypertrophy, typically bilateral, occurs in 40-65% of boys during SMR2-3 due to a relative excess of estrogenic stimulation.Growth acceleration begins in early adolescence for both sexes, but peak growth velocities are not reached until SMR3-4. Boys typically peak 2-3 yr later than girls, begin this growth at a later SMR stage (Fig. 104-5), and continue their linear growth for approximately 2-3 yr after girls have stopped. The asymmetric growth spurt begins distally, with enlargement of the hands and feet, followed by the arms and legs, and finally, the trunk and chest, giving young adolescents a gawky appearance. Rapid enlargement of the larynx, pharynx, and lungs leads to changes in vocal quality, typically preceded by vocal instability (voice cracking). Elongation of the optic globe often results in nearsightedness. Dental changes include jaw growth, loss of the final deciduous teeth, and eruption of the permanent cuspids, premolars, and finally, molars (Chapter 299). Orthodontic appliances may be needed, secondary to growth exacerbations of bite disturbances.
Self-Concept
This exposure may cause girls to develop a distorted sense of femininity, and they may be at risk for viewing themselves as overweight, leading to eating disorders and depression (Chapter 26). Similarly, boys may have difficulties with self-image. Images of masculinity may be confusing, leading to self-doubt, insecurity, and misleading conceptions about male behavior. Adolescents who develop earlier than their peers, especially girls, may have higher rates of school difficulty, body dissatisfaction, and depression. These adolescents look like adults and may have adult expectations placed on them, but are not cognitively or psychologically mature.
Middle Adolescence
Biologic Development
Growth accelerates above the prepubertal rate of 6-7 cm (3 in) per year during middle adolescence. In the average girl, the growth spurt peaks at 11.5 yr at a top velocity of 8.3 cm (3.8 in) per year and then slows to a stop at 16 yr (see Fig. 104-5). In the average boy, the growth spurt starts later, peaks at 13.5 yr at 9.5 cm (4.3 in) per year, and then slows to a stop at 18 yr. Weight gain parallels linear growth, with a delay of several months, so that adolescents seem first to stretch and then to fill out. Muscle mass also increases, followed approximately 6 mo later by an increase in strength; boys show greater gains in both. Lean body mass, approximately 80% in the average prepubertal child, increases to 90% in boys and decreases to 75% in girls as subcutaneous fat accumulates.
Boys with SMR3 pubic hair and SMR4 genitals normally have their peak growth spurts ahead of them; girls at the same SMR are usually past their peaks (see Figs. 104-3 and 104-4). Widening of the shoulders in boys and the hips in girls is also hormonally determined. Other changes include a doubling in heart size and lung vital capacity. Blood pressure, blood volume, and hematocrit rise, particularly in boys. Androgenic stimulation of sebaceous and apocrine glands results in acne and body odor. Physiologic changes in sleep patterns and requirements may be mistaken for laziness; adolescents have difficulty falling asleep and waking up, especially for early school start times as opposed to typical self-regulated or preferred sleep schedules.



