Acute abdominal pain is very common. It is important to quickly assess whether surgical intervention is required, as some important surgical conditions present as an acute abdomen.
Acute Appendicitis
This occurs in 3–4 per 1000 children and can present at any age, especially beyond 5 years of age, and is difficult to diagnose in very young children. In older children the pain is typically periumbilical and moves over a few hours to the right iliac fossa. There is loss of appetite and a reluctance to move. The most reliable signs are pain on movement and tenderness in the right iliac fossa due to peritonitis. There is often constipation, occasionally diarrhoea and vomiting and usually a low-grade fever. Investigations may show leucocytosis and neutrophilia. Urine should be checked to exclude infection. Abdominal radiograph is not helpful but CT scan or ultrasound is performed if the diagnosis is in doubt or an appendix abscess is suspected.
The differential diagnosis of iliac fossa pain includes:
- Mesenteric adenitis
- Gastroenteritis
- Constipation
- Urinary tract infection
- Henoch–Schönlein purpura (HSP)
- Inflammatory bowel disease
- Ovarian pain
- Ectopic pregancy
- Pylelonephritis.
Treatment is appendicectomy. This can be performed laparoscopically and has an excellent prognosis. Perforation is commoner in children. If peritonitis has occurred there may be severe illness and adhesions may later cause bowel obstruction.
Intussusception
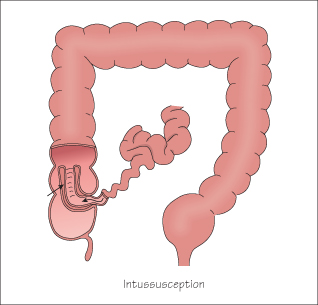
Intussusception is the telescoping of one part of bowel into another; usually the ileum into the caecum (75%). It is commonest between 3 and 24 months; only 10% occur in children >3 years of age. Enlarged lymphatics may form the leading edge of the intussusception and this often follows a viral infection (adenovirus or rotavirus). Very rarely it is due to a pathological lesion such as a polyp or lymphoma or as a complication of HSP.
The child presents with episodic screaming and pallor and between episodes may appear well. There may be shock or dehydration. Passage of blood and mucus in the stool (‘redcurrant jelly’ stool) occurs in 75%, but is a late sign. A sausage-shaped mass may be palpable.
Abdominal radiograph may show the rounded edge of the intussusception against the gas-filled lumen of the distal bowel, with signs of proximal bowel obstruction. Ultrasound can confirm the presence of bowel within bowel—the ‘doughnut sign’. The intussusception can often be reduced by an air or barium enema. If this fails or there is evidence of peritonitis then a laparotomy is required.
Children still die of intussusception because it can present non-specifically and the diagnosis is not always considered.
Other Surgical Causes of Acute Abdominal Pain
Ovarian Cysts
Ovarian cysts can be present even in prepubertal children and are present in 20% of teenage girls. They are usually asymptomatic but can cause severe pain with torsion, rupture or bleeding into the cyst. Mittleschmerz occurs in mid menstrual cycle due to rupture of a follicular cyst.
Volvulus
This is torsion of a malrotated intestine and presents with severe abdominal pain and bilious vomiting. Urgent surgery is required to untwist the volvulus and treat the underlying malrotation. If missed, the bowel may infarct.
Renal, Ureteric and Biliary Stones
Stones cause severe colicky pain but are relatively rare in childhood, unless there is an underlying metabolic or haemolytic disorder.
Non-Surgical Causes of Acute Abdominal Pain
- Colicky abdominal pain is a very common feature of gastroenteritis (Chapter 30) and may precede vomiting and diarrhoea by some hours.
- In sexually active girls, pelvic inflammatory disease and ectopic pregnancy should be considered. A pregnancy test and ultrasound may be indicated.
- Urinary tract infection, (pyelonephritis) can cause abdominal pain more than dysuria (see Chapter 34).
- Diabetic ketoacidosis may characteristically cause abdominal pain and vomiting (Chapter 18).
- Lower lobe pneumonia may cause pain referred to the abdomen.
- HSP causes abdominal pain due to widespread vasculitis (Chapter 53) and these children are at risk of intussusception.
Abdominal pain is a common symptom of anxiety and school refusal (Chapter 12).
Mesenteric Adenitis
Mesenteric adenitis is caused by inflammation of intra-abdominal lymph nodes following an upper respiratory tract infection or gastroenteritis. The enlarged nodes cause acute pain which can mimic appendicitis, but there is no peritonism or guarding and there may be evidence of infection in the throat or chest. It is a diagnosis of exclusion and treatment is with simple analgesia.
< div class='tao-gold-member'>



