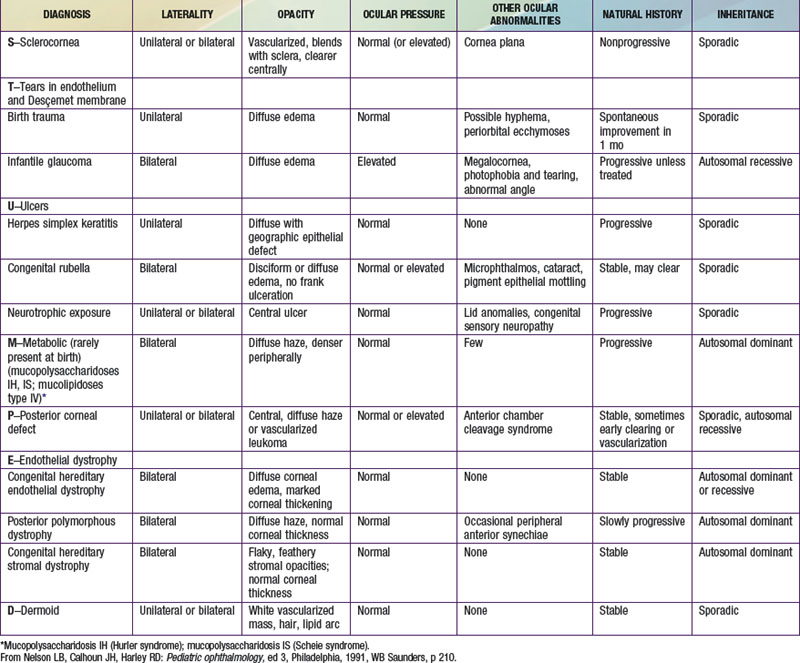
Chapter 619 Abnormalities of the Cornea Scott E. Olitsky, Denise Hug, Laura S. Plummer, Merrill Stass-Isern Megalocornea This is a nonprogressive symmetric condition characterized by an enlarged cornea (>12 mm in diameter) and an anterior segment in which there is no evidence of previous or concurrent ocular hypertension. High myopia is frequently present and may lead to reduced vision. A frequent complication is the development of lens opacities in adult life. All modes of inheritance have been described, although X-linked recessive is the most common; therefore, this disorder more commonly affects males. Systemic abnormalities that may be associated with megalocornea include Marfan syndrome, craniosynostosis, and Alport syndrome. The cause of the enlargement of the cornea and the anterior segment is unknown, but possible explanations include a defect in the growth of the optic cup and an arrest of congenital glaucoma. The region on the X chromosome responsible for this disorder has been identified. Pathologic corneal enlargement caused by glaucoma is to be differentiated from this anomaly. Any progressive increase in the size of the cornea, especially when accompanied by photophobia, lacrimation, or haziness of the cornea, requires prompt ophthalmologic evaluation. Microcornea Microcornea, or anterior microphthalmia, is an abnormally small cornea in an otherwise relatively normal eye. It may be familial, with transmission being dominant more often than recessive. More commonly, a small cornea is just 1 feature of an otherwise developmentally abnormal or microphthalmic eye; associated defects include colobomas, microphakia, congenital cataract, glaucoma, and aniridia. Keratoconus This is a disease of unclear pathogenesis characterized by progressive thinning and bulging of the central cornea, which becomes cone shaped. Although familial cases are known, most cases are sporadic. Eye rubbing and contact lens wear have been implicated as pathogenic, but the evidence to support this is equivocal. The incidence is increased in individuals with atopy, Down syndrome, Marfan syndrome, and retinitis pigmentosa. Most cases are bilateral, but involvement may be asymmetric. The disorder usually presents and progresses rapidly during adolescence; progression slows and stabilizes when patients reach full growth. Desçemet membrane may occasionally be stretched beyond its elastic breaking point, causing an acute rupture in the membrane with resultant sudden and marked corneal edema (acute hydrops) and decrease in vision. The corneal edema resolves as endothelial cells cover the defective area. Some degree of corneal scarring occurs, but the visual acuity is often better than before the initial incident. Signs of keratoconus include Munson sign (bulging of the lower eyelid on looking downward) and the presence of a Fleischer ring (a deposit of iron in the epithelium at the base of the cone). Corneal transplantation is indicated if satisfactory visual acuity cannot be attained with the use of contact lenses. Neonatal Corneal Opacities Loss of the normal transparency of the cornea in neonates may occur secondary to either intrinsic hereditary or extrinsic environmental causes (Table 619-1). Table 619-1 STUMPED: DIFFERENTIAL DIAGNOSIS OF NEONATAL CORNEAL OPACITIES Sclerocornea In sclerocornea, the normal translucent cornea is replaced by sclera-like tissue. Instead of a clearly demarcated cornea, white, feathery, often ill-defined and vascularized tissue develops in the peripheral cornea, appearing to blend with and extend from the sclera. The central cornea is usually clearer, but total replacement of the cornea with sclera may occur. The curvature of the cornea is often flatter, similar to the sclera. Potentially coexisting abnormalities include a shallow anterior chamber, iris abnormalities, and microphthalmos. This condition is usually bilateral. In approximately 50% of cases, a dominant or recessive inheritance has been described. Sclerocornea has been reported in association with numerous systemic abnormalities including limb deformities, craniofacial defects, and genitourinary disorders. In generalized sclerocornea, early keratoplasty should be considered in an effort to provide vision. Peters Anomaly Peters anomaly is a central corneal opacity (leukoma) that is present at birth (Fig. 619-1 Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Rumination, Pica, and Elimination (Enuresis, Encopresis) Disorders Adolescent Pregnancy Neisseria gonorrhoeae (Gonococcus) Blastomycosis (Blastomyces dermatitidis) Stay updated, free articles. Join our Telegram channel Join Tags: Nelson Textbook of Pediatrics Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on Abnormalities of the Cornea Full access? Get Clinical Tree
Chapter 619 Abnormalities of the Cornea Scott E. Olitsky, Denise Hug, Laura S. Plummer, Merrill Stass-Isern Megalocornea This is a nonprogressive symmetric condition characterized by an enlarged cornea (>12 mm in diameter) and an anterior segment in which there is no evidence of previous or concurrent ocular hypertension. High myopia is frequently present and may lead to reduced vision. A frequent complication is the development of lens opacities in adult life. All modes of inheritance have been described, although X-linked recessive is the most common; therefore, this disorder more commonly affects males. Systemic abnormalities that may be associated with megalocornea include Marfan syndrome, craniosynostosis, and Alport syndrome. The cause of the enlargement of the cornea and the anterior segment is unknown, but possible explanations include a defect in the growth of the optic cup and an arrest of congenital glaucoma. The region on the X chromosome responsible for this disorder has been identified. Pathologic corneal enlargement caused by glaucoma is to be differentiated from this anomaly. Any progressive increase in the size of the cornea, especially when accompanied by photophobia, lacrimation, or haziness of the cornea, requires prompt ophthalmologic evaluation. Microcornea Microcornea, or anterior microphthalmia, is an abnormally small cornea in an otherwise relatively normal eye. It may be familial, with transmission being dominant more often than recessive. More commonly, a small cornea is just 1 feature of an otherwise developmentally abnormal or microphthalmic eye; associated defects include colobomas, microphakia, congenital cataract, glaucoma, and aniridia. Keratoconus This is a disease of unclear pathogenesis characterized by progressive thinning and bulging of the central cornea, which becomes cone shaped. Although familial cases are known, most cases are sporadic. Eye rubbing and contact lens wear have been implicated as pathogenic, but the evidence to support this is equivocal. The incidence is increased in individuals with atopy, Down syndrome, Marfan syndrome, and retinitis pigmentosa. Most cases are bilateral, but involvement may be asymmetric. The disorder usually presents and progresses rapidly during adolescence; progression slows and stabilizes when patients reach full growth. Desçemet membrane may occasionally be stretched beyond its elastic breaking point, causing an acute rupture in the membrane with resultant sudden and marked corneal edema (acute hydrops) and decrease in vision. The corneal edema resolves as endothelial cells cover the defective area. Some degree of corneal scarring occurs, but the visual acuity is often better than before the initial incident. Signs of keratoconus include Munson sign (bulging of the lower eyelid on looking downward) and the presence of a Fleischer ring (a deposit of iron in the epithelium at the base of the cone). Corneal transplantation is indicated if satisfactory visual acuity cannot be attained with the use of contact lenses. Neonatal Corneal Opacities Loss of the normal transparency of the cornea in neonates may occur secondary to either intrinsic hereditary or extrinsic environmental causes (Table 619-1). Table 619-1 STUMPED: DIFFERENTIAL DIAGNOSIS OF NEONATAL CORNEAL OPACITIES Sclerocornea In sclerocornea, the normal translucent cornea is replaced by sclera-like tissue. Instead of a clearly demarcated cornea, white, feathery, often ill-defined and vascularized tissue develops in the peripheral cornea, appearing to blend with and extend from the sclera. The central cornea is usually clearer, but total replacement of the cornea with sclera may occur. The curvature of the cornea is often flatter, similar to the sclera. Potentially coexisting abnormalities include a shallow anterior chamber, iris abnormalities, and microphthalmos. This condition is usually bilateral. In approximately 50% of cases, a dominant or recessive inheritance has been described. Sclerocornea has been reported in association with numerous systemic abnormalities including limb deformities, craniofacial defects, and genitourinary disorders. In generalized sclerocornea, early keratoplasty should be considered in an effort to provide vision. Peters Anomaly Peters anomaly is a central corneal opacity (leukoma) that is present at birth (Fig. 619-1 Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Rumination, Pica, and Elimination (Enuresis, Encopresis) Disorders Adolescent Pregnancy Neisseria gonorrhoeae (Gonococcus) Blastomycosis (Blastomyces dermatitidis) Stay updated, free articles. Join our Telegram channel Join Tags: Nelson Textbook of Pediatrics Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on Abnormalities of the Cornea Full access? Get Clinical Tree