Abnormal Umbilical Vessels
Anne Kennedy, MD
DIFFERENTIAL DIAGNOSIS
Common
Single Umbilical Artery
Hypoplastic Umbilical Artery
Velamentous Cord
Less Common
Persistent Right Umbilical Vein
Fused Umbilical Cords
Conjoined Twins
Twin Reversed Arterial Perfusion
Rare but Important
Body Stalk Anomaly
Umbilical Cord Aneurysms
Umbilical Vein Varix
Umbilical Artery Aneurysm
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Cord assessment is an important part of all obstetric scans
Look at abdominal cord insertion site
Look at placental cord insertion site
Evaluate cord structure
How many vessels are there?
Is the cord length normal?
Is there an appropriate amount of “twist” to the vessels?
Follow umbilical vein
Normal course of umbilical vein (UV) is to enter left lobe of liver medial to gallbladder
UV connects with left portal vein (LPV)
LPV connects with inferior vena cava via ductus venosus
Helpful Clues for Common Diagnoses
Single Umbilical Artery
Seen best on free loop of cord cross-section
Only 1 artery adjacent to fetal bladder
Single umbilical artery (SUA) is larger than normal UA (i.e., in a 3-vessel cord)
Carries twice the blood volume
15% develop intrauterine growth restriction (IUGR)
Look for additional fetal anomalies
50% risk of aneuploidy if other anomalies in addition to SUA
Hypoplastic Umbilical Artery
Within spectrum of SUA
Asymmetry in size of umbilical arteries
One artery smaller than the other adjacent to bladder
Velamentous Cord
Submembranous cord insertion (i.e., umbilical cord inserts onto membranes not placental disc)
Often adjacent to placenta
Cord vessels are dilated due to lack of support from surrounding tissue
Submembranous vessels are extremely fragile
Associated with succenturiate lobe of placenta, placenta previa, twin gestations
Vasa previa: Submembranous fetal vessels cross cervical os
If membranes rupture fetus can exsanguinate
60-80% fetal mortality if diagnosis missed
Helpful Clues for Less Common Diagnoses
Persistent Right Umbilical Vein
Associated with SUA in most cases
May be either intrahepatic or extrahepatic
Intrahepatic: UV passes to right (lateral) of gallbladder (GB) curving toward stomach
GB medially displaced
GB transversely oriented
UV fuses with left portal vein
Extrahepatic: UV bypasses liver and portal system running anterior to liver
Drains into systemic veins
Associated with aneuploidy
Associated with multiple anomalies
Fused Umbilical Cords
Abnormal number of cord vessels in excess of the usual 3
Most commonly seen with conjoined twins
Described in monoamniotic twins where cords fuse proximal to placental insertion site
Differentiate from cord knot in monoamniotic twins
Cord vessels appear to “branch” within the knot
In fused cords, the vessels are tubular with the usual helical twist but no entanglement
Fetuses may lie close to each other but do not have contiguous skin covering
Conjoined Twins
Monochorionic twin gestation
Contiguous skin covering between fetuses
Variable cord vascular anomalies described
Most common is fused cord with 6 vessels (2 arteries and 1 vein from each fetus)
Twin Reversed Arterial Perfusion
Monochorionic twin gestation
Pump twin structurally normal
“Acardiac” twin dysmorphic with extensive soft tissue edema
Single umbilical artery in 66% of acardiac twins
Hallmark of diagnosis is abnormal direction of flow in UA
Normal UA flow is toward placenta, away from fetus
In TRAP sequence UA flow is away from placenta, into anomalous fetus
Helpful Clues for Rare Diagnoses
Body Stalk Anomaly
Absent or very short umbilical cord
Vessels seen running between placental surface and fetal torso
Large thoraco-abdominal wall defect without covering membrane
Scoliosis is a prominent feature
Fixed fetal/placental relationship essential for this diagnosis
Umbilical Cord Aneurysms
Umbilical Vein Varix
Focal dilatation of UV > 9 mm diameter or varix diameter 50% > intrahepatic portion of UV
Cyst-like space in upper abdomen with venous flow on Doppler
Rarely seen in free-floating loops of cord
Evaluate with color and spectral Doppler
Increasing turbulence on spectral or incomplete filling on color concerning for thrombus
Associated with increased venous pressure and hydrops
Umbilical Artery Aneurysm
Saccular dilatation of umbilical artery
Usually near placental end of cord
Spectral Doppler shows arterial waveform
May have arteriovenous fistula to umbilical vein
Look for associated anomalies (associated with trisomy 18)
Other Essential Information
SUA may be an incidental finding but may be associated with multiple anomalies
Careful fetal assessment required for structural malformation
If additional malformations seen, risk of aneuploidy up to 50%
Even if no other findings fetus at risk for IUGR
Follow up growth in 3rd trimester
Consider Doppler studies of cord vessels
Increased systolic to diastolic ratio associated with increased risk of IUGR
Image Gallery
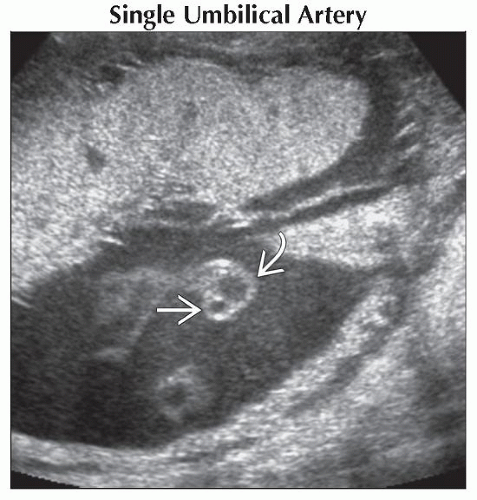 Ultrasound shows only 2 vessels in the free-floating loops of the cord. The larger vessel is the UV  , and the smaller is the UA , and the smaller is the UA  . The fetus was otherwise normal. . The fetus was otherwise normal. |
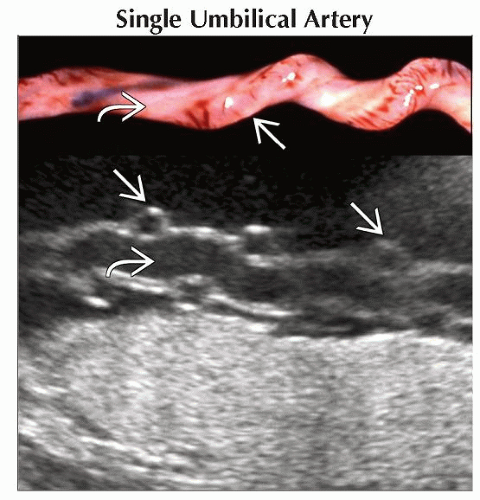 Ultrasound, with clinical correlation, shows a 2-vessel cord with a single umbilical artery  wrapping around the vein wrapping around the vein  . . |
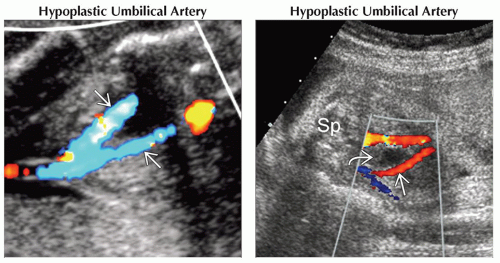 (Left) Axial color Doppler ultrasound at the fetal bladder shows asymmetric size of the umbilical arteries
 . Three vessels were present in the cord, with one artery significantly smaller than the other. (Right) Axial oblique color Doppler ultrasound shows 2 umbilical arteries adjacent to the bladder . Three vessels were present in the cord, with one artery significantly smaller than the other. (Right) Axial oblique color Doppler ultrasound shows 2 umbilical arteries adjacent to the bladder  . The left . The left  is smaller than the right (Sp = spine). The left artery is more often hypoplastic or absent than the right. is smaller than the right (Sp = spine). The left artery is more often hypoplastic or absent than the right.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|