Aetiology
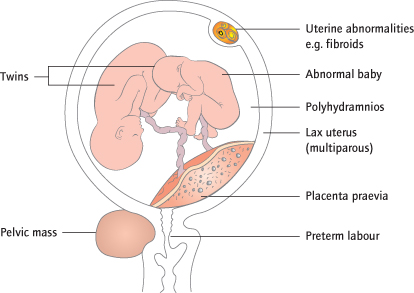
Preterm labour is more commonly complicated by an abnormal lie than labour at full term. Circumstances that allow more room to turn, e.g. polyhydramnios [→ p.164] or high parity (more lax uterus), are the most common causes, frequently resulting in an ‘unstable’ or continually changing lie. Conditions that prevent turning, e.g. fetal and uterine abnormalities and twin pregnancies, may also cause persistent transverse lie, as may conditions that prevent engagement, e.g. placenta praevia and pelvic tumours or uterine deformities (Fig. 26.2). Unstable lie in nulliparous women is rare.
Complications
If the head or breech cannot enter the pelvis, labour cannot deliver the fetus. An arm or the umbilical cord (Fig. 26.3) may prolapse when the membranes rupture, and if neglected the obstruction eventually causes uterine rupture. Both fetus and mother are therefore at risk.

Management
No action is required for transverse or unstable lie before 37 weeks unless the woman is in labour. After 37 weeks, the woman is usually admitted to hospital in case the membranes rupture and an ultrasound scan performed to exclude particular identifiable causes, notably polyhydramnios and placenta praevia. External cephalic version (ECV [→ p.228]) is unjustified because the fetus usually turns back. If spontaneous version occurs and persists for more than 48 h the mother discharged. In the absence of pelvic obstruction, an abnormal lie will usually stabilize before 41 weeks. At this stage, or if the woman is in labour, the persistently abnormal lie is delivered by Caesarean, but in expert hands ECV and then amniotomy (stabilizing induction) is an alternative.
Breech Presentation
Definitions and Epidemiology
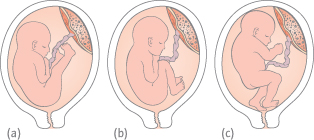
The presentation refers to the part of the fetus that occupies the lower segment of the uterus or the pelvis. Presentation of the buttocks is breech presentation (Fig. 26.4). It occurs in 3% of term pregnancies, but, like the abnormal lie, is common earlier in the pregnancy and is therefore more common (25%) if labour occurs prematurely. The extended breech (70%) has both legs extended at the knee. The flexed breech (15%) has both legs flexed at the knee. In the footling breech (15%, more common if preterm) one or both feet present below the buttocks.
Aetiology
No cause is found with most. A previous breech presentation has occurred in 8%. Prematurity is commonly associated with breech presentation. Conditions that prevent movement, such as fetal and uterine abnormalities or twin pregnancies, or that prevent engagement of the head, such as placenta praevia, pelvic tumours and pelvic deformities are more common (Fig. 26.2).
Diagnosis
Breech presentation is commonly (30%) missed, but diagnosis is only important from 37 weeks or if the patient is in labour. Upper abdominal discomfort is common: the hard head is normally palpable and ballottable at the fundus. Ultrasound confirms the diagnosis, helps detection of a fetal abnormality, pelvic tumour or a placenta praevia and ensures the prerequisites for ECV are met.
Complications
Perinatal and long-term morbidity and mortality are increased. Fetal abnormalities are more common, but even ‘normal’ breech babies have higher rates of long-term neurological handicap (BMJ 1996; 312
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


