Abnormal Cardiac Axis
Anne Kennedy, MD
DIFFERENTIAL DIAGNOSIS
Common
Chest Mass
Congenital Diaphragmatic Hernia
Cystic Adenomatoid Malformation
Bronchopulmonary Sequestration
Pleural Effusion
Teratoma
Cardiac
Chamber Asymmetry
Conotruncal Malformation
Heterotaxy, Cardiosplenic Syndromes
Less Common
Pulmonary Agenesis
Rare but Important
Ectopia Cordis
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Important to have systematic approach
In all OB scans check fetal orientation
Which is the fetal anatomic left and right?
Check position of stomach
Check position of cardiac apex
Stomach and cardiac apex should both be on the left
If both on right, likely complete situs inversus with good prognosis
If opposite sides, likely heterotaxy syndrome
Strong association with complex congenital heart disease
Normal four chamber view is seen on an axial image of the chest
Ribs should be symmetric and C-shaped
Normal cardiac axis is 35° to 45°
Draw a line from spine to sternum
Draw a line along axis of intraventricular septum
If axis is abnormal
Does the heart appear displaced within the thorax?
May be “pushed” to one side by a mass
May be “pulled” to one side if lung small or absent
Ectopia cordis implies heart situated outside thorax
Intra-abdominal
Extrathoracic
Is the internal cardiac structure normal?
Normal right and left atria
Normal right and left ventricles
Normal outflow tracts crossing as they exit the heart
Atrioventricular concordance
Ventriculoarterial concordance
Helpful Clues for Common Diagnoses
Congenital Diaphragmatic Hernia
Stomach/intestine ± liver in chest
Heart displaced away from side of hernia
In bilateral hernias, there may be minimal cardiac shift
Look for peristalsis within chest
Look for “bucket handle” motion of diaphragm on coronal view
Strong association with aneuploidy
Cystic Adenomatoid Malformation
Chest mass with perfusion from pulmonary artery branches
May be uniformly echogenic to multicystic depending on type
Heart displaced away from mass
Bronchopulmonary Sequestration
Echogenic mass with perfusion from aorta
Usually on left, with cardiac shift to the right side
Pleural Effusion
Large solitary effusion may displace heart
Look for floating lung
Differentiate from pericardial effusion
Surrounds heart, displaces lung posteriorly
Teratoma
Complex cystic/solid mass ± calcifications
Chamber Asymmetry
Which chamber is abnormal? Or is it a single ventricle heart?
Right heart enlargement
Shunt lesions with increased venous return
Incipient hydrops
Severe placental insufficiency
Left heart outflow obstruction
Small right ventricle (RV)
Pulmonary atresia/stenosis (RV can also be normal)
Left dominant unbalanced atrioventricular septal defect (AVSD)
Small left ventricle (LV)
Hypoplastic left heart syndrome (may have poorly functioning echogenic LV in aortic stenosis with endocardial fibroelastosis)
Right dominant unbalanced AVSD
Large right atrium
Ebstein anomaly/tricuspid dysplasia
Pulmonary stenosis/atresia
Conotruncal Malformation
Four chamber view often shows normal chambers
Look at outflow tracts in every case
Single outflow: Truncus most likely if normal sized ventricles and VSD present
Parallel outflow tracts: Transposition of the great arteries or double outlet right ventricle
Large aorta overriding VSD with separate, small PA: Tetralogy of Fallot
Heterotaxy, Cardiosplenic Syndromes
Check situs in every OB scan: Cardiac apex and stomach should be on the left
Look for interrupted inferior vena cava with azygous continuation to the superior vena cava
Vessel located posterior to the aorta at the level of the diaphragm
Look for transverse, midline liver
Complex congenital heart disease
Often AV septal defect
Often single ventricle
Often abnormal outflow tracts
Systemic and pulmonary venous abnormalities
Helpful Clues for Less Common Diagnoses
Pulmonary Agenesis
Heart displaced to chest wall on side of missing lung
Diaphragm elevated but present on side of missing lung
No evidence of diaphragmatic hernia/lung mass “pushing” heart
Look for associated vertebral anomalies or congenital heart disease
Look for other features of VACTERL association
Helpful Clues for Rare Diagnoses
Ectopia Cordis
Heart in abnormal location
Look for amniotic bands if exterior to thorax
Pentalogy of Cantrell
Anterior diaphragmatic hernia
Midline abdominal wall defect
Cardiac anomalies
Defect of diaphragmatic pericardium
Low sternal defect
Other Essential Information
Prognosis in heterotaxy syndromes depends on complexity of cardiac disease
Association with complete heart block almost uniformly fatal
Prognosis in diaphragmatic hernia depends on liver position and presence of cardiac defects
“Liver up” or complex cardiac anomaly confers worse prognosis
Image Gallery
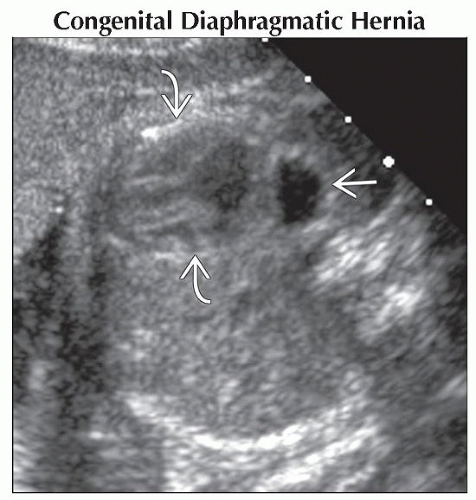 Axial ultrasound shows the stomach  behind the heart behind the heart  , which is displaced to the right. Posterior displacement of the stomach suggests “liver up” CDH, which confers poor prognosis. , which is displaced to the right. Posterior displacement of the stomach suggests “liver up” CDH, which confers poor prognosis. |
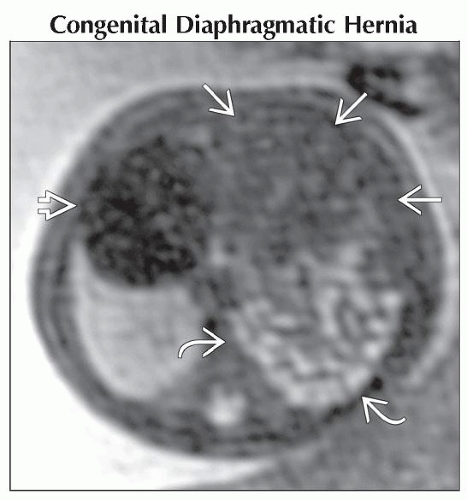 Axial T2WI MR shows bowel  and compressed lung and compressed lung  (which could be mistaken for liver) in the left chest with rightward heart (which could be mistaken for liver) in the left chest with rightward heart  displacement. Coronal views proved that the liver was not in the chest. displacement. Coronal views proved that the liver was not in the chest. |
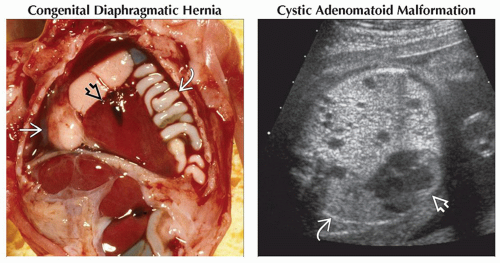 (Left) Gross pathology shows both small bowel
 and liver and liver  in the chest. The heart in the chest. The heart  is displaced to the right. (Right) Axial ultrasound shows a large, echogenic mass with small, scattered cysts consistent with a congenital cystic adenomatoid malformation. There is marked displacement of the heart is displaced to the right. (Right) Axial ultrasound shows a large, echogenic mass with small, scattered cysts consistent with a congenital cystic adenomatoid malformation. There is marked displacement of the heart  and compression of the contralateral lung and compression of the contralateral lung  . .Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|