Definition
A gait pattern in which heel contact with the ground is excluded, either completely or periodically. Toe walking may be idiopathic (i.e. of unknown cause), developmental or associated with a particular condition.
Introduction
Toe walking is the broad term used to describe the gait pattern in children who walk without making ground contact with their heels. Toe walking can be a developmental phase in young children or it may indicate an underlying pathology. Differentiation between normal or idiopathic toe walking and more serious entities is at the core of assessment of affected children.
Key Concepts
Toe walking is a common gait variant and considered normal in children under 2–3 years (Armand et al 2006, Hemo et al 2006, Kogan & Smith 2001, Stricker & Angulo 1998). Most children will have a consistent heel-to-toe pattern by the age of 2 years (Stricker & Angulo 1998).
Aetiology
The cause of idiopathic toe walking (ITW) is largely unknown but a family history is attributed in 30–71% of cases (Eiff & Steiner 2006). An increased number of type 1 muscle fibres in gastrocnemius bellies have been implicated histologically (Stricker & Angulo 1998).
Prevalence
The incidence in the general population is not known, but has been estimated to occur in 7–24% of normal children (Sobel et al 1997).
Key Concepts
The key issue when dealing with a child presenting as a toe walker is to determine whether the presentation is idiopathic or associated with specific pathology, especially cerebral palsy or muscular dystrophy.
Diagnosis
This distinction is the nub of diagnosis and future treatment considerations.
Checklist for children with cerebral palsy
• Spasticity, brisk reflexes.
• Premature term birth history.
• Low birth weight.
• Late motor milestones.
• Knee flexion at heel strike.
Checklist for children with muscular dystrophy
• Falls increase with age.
• Get up from floor in a climbing pattern (Gower’s sign; Sutherland et al 1981).
• Extensor weakness (Gaudreault et al 2007).
• Reduced ankle dorsiflexion.
Classification
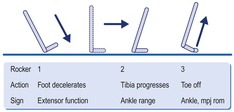
Idiopathic toe walking (ITW) has recently been classified based on a gait analysis severity scale (Alvarez et al 2007). The classification system utilizes the ankle rocker model (Perry et al 2003) to delineate three sub-types of ITW (Table 11.1, Fig. 11.1). Foot slap indicates inadequate extensor function to the control the first rocker. Lack of sagittal plane ankle range disturbs the second rocker and is commonly indicated by an early lift of the heel, flattening of the foot and increased angle of foot abduction. The third rocker requires timed firing of the triceps surae to achieve ankle plantarflexion and forward propulsion. There must also be a stable and adequate range of motion available at the first metatarsophalangeal joint. Gait was assessed to visualize three main criteria:
| ITW = idiopathic toe walking. | ||||||
| Diagnosis of ITW type directs the clinician’s decisions about treatment of these children. | ||||||
| ITW/analysis | Kinematic | Kinematic | Kinetic | Clinical | ||
|---|---|---|---|---|---|---|
| Type | First rocker present | Early third rocker present | Predominant first ankle plantarflexion moment | Ankle range dorsiflexion | Treatment indicated | |
| 1 Mild | Yes | No | No | Normal | No | |
| 2 Moderate | Yes or no | Yes or no | No | Normal or reduced | No, review | |
| 3 Severe | No | Yes | Yes | Reduced or negative | Yes | |
Type 1. Mild
Presence of the first ankle rocker (kinematic):
• normally occurs from heel strike to maximum ankle plantarflexion with loading in the first 12% of the gait cycle
• present if initial ankle angle is greater than 5° plantarflexion.
Type 2. Moderate
Presence of an early third ankle rocker (kinematic):
• normally occurs after 40% gait cycle when ankle plantarflexion ends heel contact at the completion of the second rocker phase
• present if third rocker occurs before or at 30% of the gait cycle.
Type 3. Severe
Predominant first ankle moment (kinetic):
• compares the initial stance ankle plantarflexion moment with the peak ankle plantarflexion moment of late stance
• present if the first ankle plantarflexion moment is greater than the second ankle plantarflexion moment, indicative of increasing ankle plantarflexion in early stance (Fig. 11.1).
Using this classification system in a study of the gait patterns of 133 children (266 feet) with ITW (average age 8 years), the following type proportions were found:
| Type 1 (mild) | 40 feet |
| Type 2 (moderate) | 129 feet |
| Type 3 (severe) | 90 feet |
| (Seven feet were unable to be classified; Alvarez et al 2007). | |
Differential diagnosis
Cerebral palsy, muscular dystrophy, clubfoot deformity, autism, short Achilles tendon and neuropathy have all been associated with toe walking gait patterns (Armand et al 2006, Hemo et al 2006, Hirsch & Wagner 2004). Idiopathic toe walking (ITW) is diagnosed by excluding other underlying pathologies and remains the term used to describe a toe–toe gait pattern (Armand et al 2006, Kogan & Smith 2001). Children with ITW typically walk on their toes but are usually able to make heel contact when requested.
It can be especially difficult to distinguish ITW from diplegia (Kogan & Smith 2001, Policy et al 2001, Sobel et al 1997). However, children with ITW usually have normal milestones for walking in comparison to children with diplegia, who begin to walk later (Kogan & Smith 2001). In addition, children with ITW display maximum knee extension at heel contact as opposed to children with cerebral palsy who have a flexed knee at heel strike (Eiff & Steiner 2006).
Typical clinical picture
Parents usually present with concern about their child’s toe walking after the age of 3 years, when very few other children exhibit this gait pattern and when it becomes constant rather than transient. There may be peer pressure issues when children are at school. Teachers, grandparents, friends and neighbours may also comment on the child’s gait. Toe walking may be seen as cute ‘twinkle-toes’ in little children, but can become a source of embarrassment and grounds for teasing in older children.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


