Definition of embryology and fetal development 15
Introduction 15
Fetal period 21
The foot and lower limb at birth 28
Summary 29
Definition of embryology and fetal development
The period of in utero development from conception to the eighth gestational week (of the embryo) and henceforth, until birth (of the fetus).
Introduction
As podiatrists, it is important to have a fundamental understanding of the physical development of the foot and leg from conception to birth and beyond. This chapter presents a very basic précis of the physiological and neurological developments that occur to influence the eventual lower limb. It is wise to regard this chapter as a working guide, and your are advised to expand your knowledge by looking at the work listed in ‘Further reading’.
This chapter will address the development of the foot during the embryonic and fetal periods and summarizes the expected morphology which accompanies full-term (versus pre-term) gestation. Many of the pathologies later encountered have their origins in aberrant development within the embryonic period and beyond.
Embryonic period
The embryonic period includes the germinal period (conception + 14 days), but technically begins at the third week post-conception and ends at the end of week 8 (Payne & Isaacs 2008).
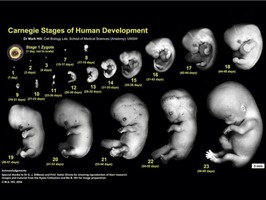
From the time of fertilization of the ovum, myriad changes occur to convert the pre-lower limb buds to the eventual individual foot bones which are, in the main, present at the end of gestation. The embryonic period is defined as the first seven post-ovulatory weeks (Tachdjian 1997) and is divided into 23 stages or horizons, each of which corresponds to a developmental stage of the embryo (as described by Streeter, Carnegie, see Further reading; Sarrafian 1993). These stages are based on the external and/or internal morphological development of the embryo, rather than age or size (Fig. 2.1).
The embryonic cell mass or zygote divides and differentiates to form:
• Ectoderm: forms epidermis, sensory receptors and nervous tissues
• Mesoderm: forms skeletal, connective, muscle and blood tissues
• Endoderm: inner layer which forms the respiratory and gastrointestinal tract linings.
Teratogens
The embryonic period is when the placenta, umbilical cord and amniotic fluid develop. During this period, the embryo is most susceptible to teratogens as the mother’s blood is shared with the developing embryo. Thalidomide, a tranquillizing drug, is an infamous example of teratogen exposure adversely affecting development, but common recreational drug use is also implicated, e.g. alcohol, tobacco, cannabis, cocaine (Payne & Isaacs 2008).
Specific anomalies associated with recreational drug use include:
Alcohol
• Growth retardation, craniofacial abnormalities, CNS dysfunction.
• Fetal alcohol syndome (FAS) represents a cluster of birth defects due to prenatal alcohol exposure and includes:
– ADHD (attention deficit, hyperactivity disorder)
– mental retardation
– altered facial features
– decreased physical growth
– reduced brain growth and lower IQ.
• Less severe problems are termed alcohol-related neurodevelopmental disorders (ARNDs) and include:
– slow motor development
– speech problems
– clumsiness.
The point needs to be made that there is no safe level of maternal alcohol consumption during pregnancy and as little as one daily drink has been associated with retarded growth (Payne & Isaacs 2008).
Tobacco
• The main issues associated with tobacco use during pregnancy are increased miscarriage rate, increased infant mortality, lower birth weight and twice the incidence of sudden infant death syndrome (SIDS) (Machaalani & Waters 2008). Both carbon monoxide and nicotine (two of the many tobacco by-products) contribute to fetal hypoxia.
• Postnatally, children who live in homes with prevalent smoking are more likely to exhibit respiratory diseases.
Cannabis
• While cannabis use in pregnancy has been associated with lower birth weight, there is less stringent evidence for deleterious effects than for tobacco and alcohol where the evidence is conclusive. However, it is known that THC (11-hydroxy-delta-9-tetrahydrocannabinol), the most active mind-altering ingredient, does cross the placenta and can accumulate in the fetus. Hence abstinence of cannabis use during pregnancy is advised (Klonoff-Cohen & Lam-Kruglick 2001).
Cocaine
• Whether smoked, snorted or injected the effects of cocaine are known to be among those most dangerous to the unborn baby. Premature gestational term (with all associated hazards) is increased by approximately 25% and fetal brain damage is at least four times higher than normal. As infants, cocaine-damaged babies are often both unresponsive and irritable, making care difficult and neglect or abuse more likely (Gingras et al 2004).
Common other drugs, maternal diseases and some genetic factors are summarized in Table 2.1.
| Drug | Use | Possible risks for fetus |
|---|---|---|
| Prescribed drugs | ||
| Anticoagulants | Blood clots | Miscarriage CNS, eye defects |
| Antibiotics | Infections | Altered teeth development |
| Anticonvulsants | Seizures | Neural tube defects Hand, face defects Mental retardation |
| Over-the-counter drugs | ||
| Aspirin | Pain, inflammation | Prolonged labour Increased mother’s bleeding/bleeding within baby’s skull during birth |
| Ibuprofen | Anti-inflammatory | Oligohyramnios (high use) |
| Maternal diseases | ||
| Diabetes | Macrosomia, childhood obesity CNS, spina bifida Heart defects | |
| HIV (human immunodeficiency virus) | 1. In utero: mother to fetus 2. Delivery: baby infected with blood/fluids 3. Breast milk: zidovudine has reduced HIV in susceptible cases to approx. 5% | Survival approx. 24 months 90% symptoms by 4 years Few live past 13 years (AIDS) |
| Rubella (German measles) | Congenital rubella syndrome | Deafness (80% of cases) Hepatitis, pneumonia Glaucoma, cataracts Growth/mental retardation |
| Genetic factors | ||
| Chromosome 21 (trisomy) | Down’s syndrome | |
| Chromosome 15 | Angelman syndrome Prader–Willi syndrome Marfan’s syndrome | |
| Chromosome 17 | Charcot-Marie-Tooth (1A) | |
| Chromosome 2 (deletion) | Talipes equinovarus | |
The sixth, seventh and eighth embryonic weeks are those most associated with the development of lower limb defects (Drennan 1992, Tachdjian 1985) and most major congenital abnormalities occur within the eight embryonic weeks (Payne & Isaacs 2008).
Development of the foot
The foot is derived from condensed mesenchyme (from mesoderm) projecting through the ectoderm to form the template or anlage of the foot. There are three main stages to the forming of the skeleton:
• Mesenchymal
• Cartilaginous
• Osseous.
The mesenchyme differentiates to form metatarsals, phalanges and the tarsus. Cartilage (or its precursor called procartilage) appears within the areas of condensed mesenchyme and forms a chondrified anlage. Chondrification is largely complete by the end of the embryonic period. Vascular infiltration occurs initially in the talus from the arteries within the sinus tarsi (Tachdjian 1985). The vascular supply then spreads to supply the calcaneus, navicular, cuboid, cuneiforms, metatarsals and phalanges and signals the nearing of ossification. Endochondral ossification then ensues and in a general sense progresses from forefoot to rearfoot, with the distal phalanx of the great toe being the first foot bone to ossify. The calcaneus is the first tarsal bone to ossify and the navicular the last, varying between 2 and 5 years post-birth (Evans et al 2003). The cuboid ossifies at 37 weeks’ gestation and is often used as a marker for fetal maturity. The chronological sequence of fetal foot ossification is shown in Figure 2.2.
 |
| Figure 2.2 |
The developing nervous system is evidenced in the third embryonic week when the ectoderm thickens to form the neural plate, which in turn gives rise to the neural groove and crest. Folding of the neural groove forms the neural tube which fuses and elongates in the fourth embryonic week to form the spinal cord. Much differentiation of the neural crest occurs to form various sensory and autonomic ganglia. While rapid growth of the brain occurs mid-gestation, 85% of brain growth occurs after birth (Shepherd 1995). A primitive lumbosacral plexus is formed by 5 weeks with the femoral, obturator, tibial and common peroneal nerves branching to their respective areas of the limb bud (Bareither 1995).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


