Absent Cavum Septi Pellucidi
Anne Kennedy, MD
DIFFERENTIAL DIAGNOSIS
Common
Incorrect Scan Plane
Agenesis of the Corpus Callosum
Chiari II Malformation
Severe Hydrocephalus
Less Common
Holoprosencephaly Spectrum
Alobar Holoprosencephaly
Semilobar Holoprosencephaly
Lobar Holoprosencephaly
Rare but Important
Septo-Optic Dysplasia
Schizencephaly
Syntelencephaly
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Scan technique is very important
Cavum septi pellucidi (CSP) should be the landmark for measurement of biparietal diameter and head circumference
Coronal images also helpful if fetal head position makes correct axial plane difficult
CSP seen between frontal horns inferior to corpus callosum
Cavum septi et vergae is an anatomic variant that may cause confusion
Cavum vergae is posterior continuation of CSP, usually obliterates posterior to anterior so not seen in standard 18-20 week scan
If present → elongated, larger, fluid-filled space which may be confused with interhemispheric cyst
No other abnormalities present
Normal CSP signifies normal midline brain development
If absent, significant malformation may be present though not immediately apparent
Helpful Clues for Common Diagnoses
Incorrect Scan Plane
If scan plane too high or too low CSP not seen
Fornices are normal structures which create parallel echoes inferior to normal location of CSP
CSP appears as a fluid-filled “box”: White line/black space/white line appearance
Fornices: Series of parallel black and white lines without intervening fluid-filled space
Agenesis of the Corpus Callosum
Mild ventriculomegaly or colpocephaly
Lateral ventricles are parallel instead of divergent
Coronal images show “steer horn” appearance of frontal horns
Lack of normal anterior cerebral artery branch pattern into callosomarginal and pericallosal arteries on midline sagittal view
Stenogyria: Radiating “sunburst” pattern of medial cerebral gyri
MR very helpful to look for additional brain malformations
Heterotopia, lissencephaly, gyral abnormalities
Chiari II Malformation
Ventriculomegaly with “boxy” appearance of frontal horns
“Banana” sign: Cerebellar prolapse into foramen magnum causes cerebellum to curve around brainstem
Obliteration of cisterna magna
“Lemon” sign: Bifrontal concavity
Severe Hydrocephalus
Severe hydrocephalus leads to “blown out cavum”
Fenestrations appear in leaves of septum secondary to elevated cerebrospinal fluid pressure
Eventually leaves of cavum may be so thinned as to be invisible or torn
Most likely to occur with aqueductal stenosis
Helpful Clues for Less Common Diagnoses
Alobar Holoprosencephaly
Supratentorial brain without division into cerebral hemispheres
“Rind”, “cup”, or “pancake” of cerebral tissue associated with monoventricle ± dorsal cyst
Head may be large if large dorsal cyst, or small and rounded in shape
Associated with severe facial malformation
Look for stigmata of trisomy 13
Semilobar Holoprosencephaly
Some division into cerebral hemispheres posteriorly but fusion anteriorly
Head shape often round
Look for stigmata of trisomy 13 or 18
Lobar Holoprosencephaly
Two cerebral hemispheres are formed
May be single gyrus in continuity across midline
Midline fusion anomalies seen
Fused fornices create a round “mass” in the third ventricle
Helpful Clues for Rare Diagnoses
Septo-Optic Dysplasia
Absent CSP associated with variable hypothalamic pituitary dysfunction and visual impairment
Mild dilatation of frontal horns
“Flat top” appearance to frontal horns
MR used to exclude additional malformations
Optic nerves and chiasm beyond resolution of fetal MR at present
Diagnosis is confirmed by clinical and ophthalmological evaluation of infant
Schizencephaly
Cortical defect extending from ventricular surface to pia
May be “closed” or “open”, unilateral or bilateral
Size of defect varies from very small to giant, involving most of frontoparietal cortex
Lateral ventricle on side of defect is distorted → tenting toward area of parenchymal loss
Bilateral giant open lip schizencephaly looks very similar to hydranencephaly
Key observation is that walls of a schizencephalic cleft are lined by grey matter
Important distinction as hydranencephaly is lethal
Giant open lip schizencephaly is associated with neurological impairment but is not necessarily lethal
Syntelencephaly
Considered variant of holoprosencephaly spectrum by some
Two hemispheres are present but with some fusion of the dorsal aspect of cerebral hemispheres
Most common site of fusion is posterior frontal lobe
Other Essential Information
Absent CSP is often the tip-off for underlying brain abnormality
Agenesis of corpus callosum is associated with many other brain malformation as well as innumerable syndromes
Counsel parents that outcome highly variable
Septooptic dysplasia associated with visual impairment/blindness as well as potential hypothalamic pituitary dysfunction
Image Gallery
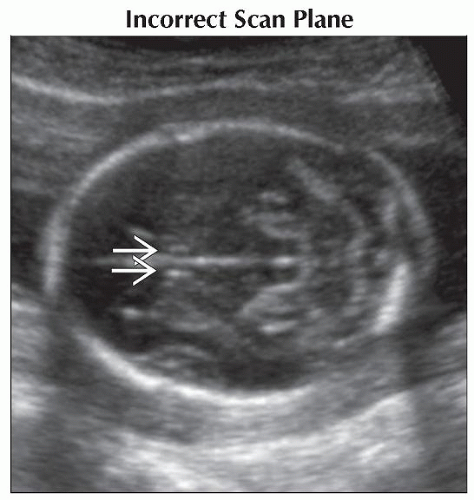 Axial oblique ultrasound of the fetal head shows the parallel lines produced by the fornices
 which lie inferior to the CSP. This should not be confused with the cavum, which should appear as a fluid-filled “box”. which lie inferior to the CSP. This should not be confused with the cavum, which should appear as a fluid-filled “box”.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|