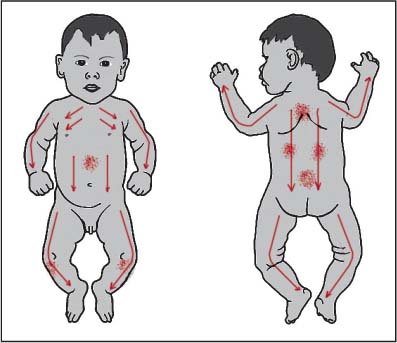
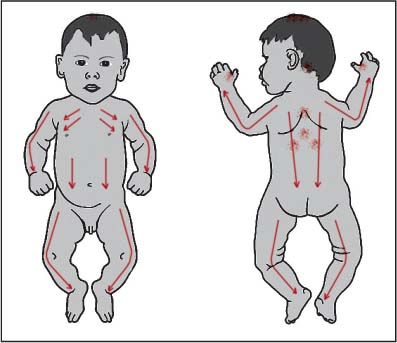
25 Weak Constitution This is a broad category that refers to the child who from birth has been having recurrent problems because of a constitutional weakness. In their description of this, Yoneyama and Mori (1964) recommend the basic core treatment and then additionally the use of moxa on BL-18 and BL-20 and possibly GV-12, which would seem to target respiratory and digestive symptoms. Shimizu (1975) differentiates three basic types of “weak constitution”: (1) the “respiratory type” with chronic respiratory symptoms, (2) the “digestive type” with chronic digestive symptoms, and (3) the “combined respiratory and digestive type” with chronic digestive and respiratory symptoms, and he provides more extensive treatment descriptions. However, as a Meridian Therapist I think that the descriptions of this category are limited. Following the patterns in Meridian Therapy, I identify four distinct weak constitution patterns, based on which I recommend differentiated treatments.1 __________________ 1 I do not follow another idea of Shimizu who describes the broad category of “kanmushi” (see Chapter 21) as a sign of weak constitution and then relates this to evolving 20th-century models of developmental stages (Shimizu 1975). I prefer to stay within the framework of traditional acupuncture as it allows both the usual core non-pattern-based root treatment approach AND a specific pattern-based treatment approach, which in my experience is usually more rapid acting than either alone. It is not only to do with how I treat patients but practically it allows two different root treatment approaches that can be used together. There are some important features associated with these weak constitutions. The problems are usually present from birth, though it is possible that they can be caused by accidents or infections after birth, starting soon after those events. There are often signs apparent in the structure and build of the child, for example being thinly muscled, small-boned, having a flat rib cage, shoulders pulled back (Shimizu 1975). The child is often very sensitive (Shimizu 1975; see discussions of sensitivity in Chapter 4) and usually has one or more symptoms present all the time. His or her problems may respond to regular medical therapy such as drug interventions, but recur soon after the therapy is discontinued. Some types of constitutional weakness can recover with treatment, other types cannot. For the latter types (such as autism, mental retardation, birth defects, severe cerebral palsy), the words of my teacher Toshio Yanagishita are very important: you have to be realistic, you cannot fix these problems, but you can help lessen their manifestations, improve quality of life, and help the parents in their continuous efforts to care for their child. There are some cases where you may feel that you really can’t do anything because the problems seem so severe. When such feelings occur, you need to deal with the following: There are a number of different ways that this can manifest: This weak constitution manifests usually in a few common ways: This usually manifests from birth with developmental problems, both mental and physical. It can also start postnatally due to, for example, accident, head trauma, infection. In this general category are included cases of mental development problems; abnormal development of the body (parts of the body that do not develop properly such as limbs, spina bifida); birth traumas leading to, for example, cerebral palsy; sequelae of infections such as loss of normal locomotor function resulting from polio infection. Thus, the general category includes cases of: The most common manifestation of this problem is severe behavioral problems starting soon after birth. Another manifestation is abnormality of the muscles, such as excessive muscle stiffness in common areas, or muscle problems resulting from growth spurts in older children. For the child who has behavioral problems, the excessive stiffness can aggravate the problems. This category thus includes cases of: Main complaints and history: From birth Mary had had severe airborne allergy problems, triggering severe asthma attacks. Since birth, she had been hospitalized six times with these asthma attacks. Each time she was discharged from the hospital with asthma medication to control the problem, she would within days be having severe asthma attacks again and would have to go to the emergency room at the hospital to be readmitted. Her mother called from the hospital on a Sunday morning to request treatment that afternoon. Mary was being discharged around noon and her mother was concerned the same problems would recur, something the doctors had said was very highly probable. It was arranged that I would meet her and Mary at the clinic straight from the hospital. Mary had no other symptoms. Sleep and appetite were generally OK. Diagnosis: While it was clear to me that Mary had a lung weak constitution (strong lung vacuity pattern), I was afraid that the general or core whole body shonishin treatment method with treatment of the lung vacuity pattern would not be fast-acting enough to prevent an attack and subsequent hospitalization. I was also concerned that Mary’s family was living in a poor housing neighborhood in the Boston area and that she was being exposed to allergens that her parents could not eliminate from their apartment.2 On the basis of these concerns I decided to try stronger measures. __________________ Treatment: For the lung constitutional weakness I decided to do okyu/direct moxa on Mary. After explaining what I planned to do and getting her mother’s permission to continue, I had the mother take Mary’s clothes off and hold Mary over her shoulder so that I could easily get to GV-12 on the back. I applied okyu (half to three-quarter rice grain size) and did nothing to control the heat or put the moxa out early. I wanted to trigger the immunological and anti-inflammatory effects of the moxa as strongly as possible. Expecting Mary to cry out or scream because of the heat of the moxa, her mother and I were very surprised when Mary instead took a deep breath as the heat of the moxa penetrated and then relaxed even more over her mother’s shoulders. I applied two more cones of moxa—Mary responded the same way each time. There was a yellow mark on the skin (which did temporarily blister). No other direct treatment was given on this visit. After Mary was dressed, I then brought out my back-up high-powered air-filtering system (which can eliminate particles, dust, and chemicals from the air).3 I explained to Mary’s mother that she could borrow the machine until she could afford to buy one herself. She should leave it running continuously in the room where Mary spends most of her time, leaving the doors open so that it additionally cleans the air in the other rooms (they lived in a small apartment). My plan was to reduce almost to zero whatever the airborne allergen was, whilst administering strong treatment to trigger a rapid change in her lung weak, allergic constitution. __________________ Mary returned the next 2 days for treatment. On each occasion treatment was applied only with moxa to GV-12. She had a small blister on this point. After the third session it was clear that Mary was, for the first time, having no allergic asthma symptoms. I then had her brought back for treatment weekly for the basic core shonishin treatment using the combination of rubbing and tapping. On the first of those treatment sessions I taught her mother how to apply the treatment daily at home. I applied weekly treatment, with the mother applying daily home treatments over the next 3 weeks. The blister completely healed with hardly a mark and Mary never had another asthma attack (at least over the few next years that I was able to track how she was doing). You must assume from the start that the child is more sensitive than other patients. Thus, trying a softer, milder treatment to begin with is generally important (review Chapter 4 for discussions of this and Chapter 7 for discussions of how to modify the core treatment). Once you have an idea of how the child responds to treatment, you can gradually increase the dose by adding in or replacing treatment methods. Figuring out a simple core non-pattern-based treatment and using that regularly is important, as is teaching the parent to start using this at home. Applying a simple pattern-based treatment according to the pattern type of constitutional weakness is also important. Here it is often useful to focus on the manifestations and symptoms to choose the pattern rather than the usual diagnostic methods of pulse and abdomen. Some patients show combined constitutional weakness, such as the patient with severe atopic dermatitis with airborne, contact, and food allergy triggers (combination of lung and spleen types); the child who has both severe eczema since birth and does not gain weight due to food allergies, poor appetite, chronic diarrhea (combination spleen and lung types); the child with mental development problems, severe gastrointestinal disturbance with food allergies (combination kidney and spleen types). Treat to improve the constitutional weakness. Where feasible, apply treatment to target symptoms. For example, for the child with mental retardation, symptomatic treatment can be difficult, but the root treatments (pattern-based and core non-pattern-based) can start creating change in daily activities and parental care of the child. Lightly stroking down the arms, legs, back, abdomen and chest (do not do this if the child has skin problems; see Chapter 19 on skin problems). Light tapping around GV-12. If the child has respiratory problems additional tapping can be applied around LU-1, and the area around ST-12 (see Fig. 25.1). Apply supplementation to LU-9 and SP-3. If the child is very rundown and weak, the skin feels too soft or loose, also supplement bilateral TB-4 or ST-36. Generally do not apply draining techniques until the child is stronger. If the child has severe skin symptoms try LU-5 and SP-9 instead of LU-9, SP-3 for the treatment of the primary pattern.4 __________________ Fig. 25.1 Lightly stroke down: • Down the back (bladder channel) • Down the abdomen (stomach channel) • Down the legs (stomach and bladder channels) • Down the arms (yang channels) • Across the chest For a lung pattern add tapping: • Around GV-12, possibly LU-1 and ST-12 regions Place a press-sphere or new press-tack to GV-12. If the symptoms in the lungs are very severe or there are recurrent infections, try applying okyu instead to GV-12. If the child has chronic skin problems, tap or apply moxa to the relevant large intestine channel points (see Chapter 19, pp. 118 and 119) instead of applying the core non-pattern-based root treatment with stroking and tapping. Shimizu’s (1975) recommended treatments for the “respiratory type” are useful to consider. Okyu/direct moxa can be applied to BL-12, GV-12, GV-10, LU-5, or LU-6, BL-23 with needling of KI-26, LU-1, BL-11, BL-17, depending on current symptoms (such as easily fatigued, easily catches cold, recurrent fevers, swollen tonsils, bronchitis, chronically swollen lymph nodes in the neck) and reactions in the acupoints. This list of acupoints offers additional options to be added over successive treatments on top of the core root treatment methods. Lightly stroking down the arms, legs, back, abdomen, and chest. Apply light tapping around GV-12, CV-12, and from GV-3 to GV-4. The area around ST-36 to ST-37 can also be lightly tapped. It can also be helpful to lightly tap around BL-18 and BL-20 (see Fig. 25.2). Apply supplementation to SP-3 and PC-7. If the child is very rundown and weak, the skin feels too soft or loose, also supplement KI-3 on the other side and bilateral ST-36. Generally do not apply draining techniques until the child is stronger. Place press-sphere to GV-12. Also place press-spheres to BL-18 on one side and BL-20 on the other. If the child is not responding sufficiently to treatment and/or the symptoms are very severe, apply okyu instead to BL-18 on one side and BL-20 on the other. The general rule for selecting side is: for boys, left BL-18, right BL-20, and girls, right BL-18, left BL-20. Although some moxa specialists recommend applying the moxa bilaterally (Irie 1980), it is better to use this contralateral treatment as it reduces the number of points you have to treat, reducing by half the amount of irritation and distress the treatment can cause. A press-sphere can be placed at CV-12 as well, if reactive. If the child has food allergies, apply moxa to the extra point uranaitei (below nei ting—ST-44) on the bottom of the foot. This is a special point for food allergies (see Chapter 16, p. 88 for the point location). Shimizu’s (1975) recommended treatments for the “digestive type” of weak constitution are useful to consider. Okyu/direct moxa can be applied to GV-12, BL-23, right BL-18, left BL-20 with needling of CV-12, KI-16, or ST-25, LR-13, ST-36, depending on current symptoms (such as poor appetite, frequent abdominal pain, diarrhea) and reactions in the acupoints. This list of acupoints offers additional options to be added over successive treatments on top of the core root treatment methods. Fig. 25.2 Lightly stroke down: • Down the back (bladder channel) • Down the abdomen (stomach channel) • Down the legs (stomach and bladder channels) • Down the arms (yang channels) • Across the chest For a spleen pattern add tapping: • Around GV-12, CV-12, GV-3, and possibly around • ST-36–ST-37, and BL-18–BL-20 Light stroking down the arms, legs, back, abdomen, and chest. Light tapping around GV-12 and GV-3. If the problems are of mental development, palpate the occipital region, if stiff, apply a light tapping there and around GV-20 (see Fig. 25.3). Apply supplementation to KI-7 and LU-8. In a kidney pattern such as this, it is not uncommon that the spleen is replete, but this is difficult to see. To counterbalance this, supplement ST-36 on the other side. If the main problems are of mental development, and the child is easily agitated, try using KI-10 and LU-5 instead of KI-7 and LU-5.5 __________________ Fig. 25.3 Lightly stroke down: • Down the back (bladder channel) • Down the abdomen (stomach channel) • Down the legs (stomach and bladder channels) • Down the arms (yang channels) • Across the chest For a kidney pattern add tapping: • Around GV-12 and/or GV-3, possibly around GV-20 and the occipital region If the child has symptoms of the upper limbs or upper part of the body, direct treatment to GV-12 if there is paralysis or problems of use of the upper limbs and around GV-3 to GV-4 if the problem is in the lower limbs. You can start gently by using press-spheres or press-tack needles. If the symptoms are stronger or the child does not respond to the milder treatment, it is better to use okyu/direct moxa on these treatment points, GV-12 for upper limbs, GV-3 or GV-4 for lower limbs. It can also be helpful to leave press-spheres at BL-23 to help reinforce your treatment of the kidneys. If the child has mental development problems, and shows signs of agitation, inspect the back of the ears behind shen men and if the skin looks less lustrous, drier, different, leave a press-sphere there.6 __________________ Fig. 25.4 Lightly stroke down: • Down the back (bladder channel) • Down the abdomen (stomach channel) • Down the legs (stomach and bladder channels) • Down the arms (yang channels) • Across the chest For a liver pattern add tapping: • Around GV-12, GV-9, possibly around GV-20, GB-20, BL-18, and LI-4 Lightly stroking down the arms, legs, back, abdomen, and chest. Apply light tapping around GV-12, GV-9, and BL-18. If the child has behavioral problems additional light tapping can be applied around GV-20, occipital region, and LI-4 (see Fig. 25.4). Apply supplementation to LR-8 and KI-10. If the child has problems of muscle pain rather than behavioral problems, try using LR-3 and KI-3 instead.7 __________________ Place a press-sphere on GV-12. If the behavioral symptoms are severe, insert needles to LI-4, GB-20 area and possibly GV-20. Following Mike Smith’s recommendation (see footnote 6), I find leaving a press-sphere on the ears behind shen men can be helpful for behavioral problems. If the condition is non-responsive or the symptoms more severe use okyu/direct moxa on GV-12, and for muscular problems GV-8. For other treatment options for manifestations of each of these weak constitution types see the following chapters: Hyodo (1986) makes the following additional recommendations for the general treatment of “weak constitution”: lightly needle and/or leave press-spheres at GV-12, GV-4, BL-18, BL-20, BL-23. For the combined “respiratory and digestive” type of weak constitution Shimizu (1975) recommends use of okyu/direct moxa on GV-12, GV-10, LU-6, BL-23, right BL-18, left BL-20 with needling of CV-12, KI-16, LR-13, ST-36, selecting acupoints on the basis of current symptoms and point reactions. The following case from my colleague Sue Pready who practices in Swindon and Cardiff in the United Kingdom, is a good example of the less common liver weak constitution type. Naomi responded well to treatment of her complicated problems. Case 2 Main complaints and history: Back pain for the last 18 months. Whilst in the midst of a growth spurt she had strained her back in physical education class, and her back did not recover. She had always been supple and slightly hyperextensive, which was agitated by the growth spurt. The pain started as pain in the heel and Achilles tendon in the right foot, traveling up to the sacroiliac joint. She also had pain in the bladder area, and found it painful to urinate, resulting in the additional problem of constipation during the last summer. The year before she had been virtually immobilized by the pain and had to be admitted to hospital. She was now under pain management at a special unit at the local hospital. While taking diclofenac she still had pain and had to skip certain school activities such as gym, and morning assembly at school. Her walking was now slightly better but still very difficult. She needed help going up and down stairs. She struggled to walk into the treatment room. The pain was worse at lunchtime when the effects of the tablets wore off. Medication: Diclofenac: half adult dose (25 mg 3 × a day for about 6 months) and paracetamol as and when needed. While the pain management strategies had been helping make her more functional, she still had pain regularly and was limited in many physical activities such as climbing stairs, running, and so on. Physical appearance: Tall for her age, slim, fair, unblinking blue eyes. Musical and intelligent, she was the youngest of three children. She had some sleep problems. Sometimes she wasn’t able to fall asleep because of the back pain, or the pain would wake her up about 3 or 4 a.m. She had been having some headaches, thought to be from the tablets she had to take. Appetite: Good mixed diet. She liked spicy food. Diagnosis: The kidney, liver, and spleen areas of the abdomen showed signs of reaction. Her pulse was slightly floating, slightly rapid and weak. Weakest pulses: liver and kidney, spleen. Conclusion: liver vacuity pattern with spleen also vacuous. Treatment: Since she was a more mature girl, the core non-pattern-based root treatment was not used. She was not particularly afraid of the treatment. Using regular needles8 supplementation was applied to left LR-8, KI-10, and right SP-3. Right ST-40 and BL-58 were drained. __________________ 8 In the style and using the methods of the Toyohari system of Meridian Therapy. Second visit—1 week later The hip had felt better for 3 days. The bladder problem was a bit easier, not hurting as much. Treatment: Using needles, left LR-8, KI-10, and right LU-9 were supplemented. Draining was applied to right SI-7. CV-6, BL-18, and BL-23 were supplemented bilaterally to support the root treatment. Light stroking was applied down the back and the backs of the legs using an enshin. A press-sphere was retained at GV-12 as home therapy. Light needling was applied to tight areas in the lateral abdomen regions and around the right hip.9 __________________ A moxa cigar was applied over the spine to warm it. Third visit—1 week later The hip felt better and she was finding it easier to walk. The bladder did not hurt as much as before starting acupuncture. Treatment: Using regular needles, left LR-8, KI-10, and right LU-9 were supplemented. Right SI-7 and GB-37 were drained. CV-6, BL-18, and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12, right BL-18, and left BL-23 to support the root treatment. Light needling was applied to tight areas in the lateral abdomen regions and around the right hip and the supraclavicular fossa region.10 __________________ Chinetsukyu/warm moxa was applied to CV-3 for the bladder. LU-7 was also supplemented with a needle to help reduce symptoms in the bladder. Fourth visit—1 week later She had found it harder to control her urination this week. She had stumbled and fallen the day before but recovered well. The hip felt all right, though she had been woken by pain two or three times this week. She was also having problems with nosebleeds (reported by her mother to be due to the diclofenac). Treatment: Examination showed a kidney vacuity pattern rather than the usual liver pattern. Using regular needles, left KI-7, LU-5, and right SP-3 were supplemented. Left SI-7 and LI-6 were drained. BL-13 and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12 and bilateral BL-23. Light needling was applied to supraclavicular fossa region. A moxa pole was applied over the spine to warm it. Fifth visit—1 week later She continued having problems with nosebleeds. Sometimes she found it difficult to fall asleep because of the hip pain. However, while the hip had been quite sore she had still been able to get down stairs by herself using the banisters as support. Urination still hurt but seemed overall easier. Treatment: Examination showed the usual liver vacuity pattern. Using regular needles, left LR-8, KI-10, and right LU-9 were supplemented, left GB-37 and BL-58 drained. Light stroking was applied down the back and the backs of the legs using an enshin. BL-18 and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12, left BL-18, and right BL-23 to support the root treatment. Light needling was applied to lower abdomen and supraclavicular fossa regions. A moxa pole was applied over the spine to warm it. Sixth visit—2 weeks later This week she had found it easier to get down stairs without help. She had had a problem with alternating diarrhea and constipation. She was able to urinate more freely now with less distress. But she had still had problems with nosebleeds the last two mornings. Because she was feeling better she had tried cutting out the lunchtime tablet of diclofenac. Treatment: An overall lighter treatment was applied: Using regular needles left LR-8, KI-10, and right LU-9 were supplemented, left GB-37 and BL-58 drained. Light needling was applied to the lower abdomen region. A mild warm moxa pole technique was applied over the abdomen for the bladder. Seventh visit—1 week later She was still having problems with nosebleeds, but had been all right without the lunchtime tablet of diclofenac. Her pain overall was better. Urination was now much better. Treatment: Treatment was similar to the previous session. Eighth visit—3 weeks later She was much better, and some days she did not take the diclofenac. Urination had improved further. Nose-bleeds were less frequent and sleep was better, but one day before this visit she had fallen over and irritated her back and hip. Treatment: Using regular needles left LR-8, KI-10, and right SP-3 were supplemented. BL-18 and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12, left BL-18, and right BL-23 to support the root treatment. Light needling was applied to lower abdomen and supraclavicular fossa regions. A moxa pole was applied over the spine to warm it. Okyu/direct moxa was applied to josen (an extra point below L5; see Chapter 16, p. 88). Ninth visit—2 weeks later She reported that she was doing well. She could now go up stairs on her own. She was walking more, had more stamina, and was coping better. Urination was still a bit uncomfortable but much easier. She was still having some problems with nosebleeds at night. She had only taken diclofenac once or twice a week. Overall sleep was better, abdominal discomfort better. Treatment: Using regular needles, left LR-8, KI-10, and right SP-3 were supplemented. BL-18 and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12, left BL-18, and right BL-23 to support the root treatment. Light needling was applied to lower abdomen and supraclavicular fossa regions. A moxa pole was applied over the spine to warm it. Okyu/direct moxa was applied to josen and BL-28. After this, the next four visits were similar as she continued improving. Fourteenth visit—4 months later She was doing much better. She had stopped taking diclofenac, occasionally needing paracetamol for pain relief. Her mobility was improving; she was now able to run up and down stairs, the hip and back were much better, and she was walking more easily. She was able to go on longer walks with the dog. Urination was satisfactory. Treatment: Using regular needles, left LR-8, KI-10, and right SP-3 were supplemented. BL-18 and BL-23 were supplemented bilaterally to support the root treatment. Press-spheres were retained at GV-12, left BL-18, and right BL-23 to support the root treatment. Light needling was applied to lower abdomen and supraclavicular fossa regions. A moxa pole was applied over the spine to warm it. Okyu/direct moxa was applied to josen, BL-28, GV-12. Fifteenth visit—6 weeks later She had had a review at the hospital the previous Friday—everything was fine. She had grown 4 cm in the last 4 months. She had not taken diclofenac for a long time. Her sleep was generally satisfactory. Urination was also much better. The day before the visit she had had a slight setback, playing netball, and had a pain in the left foot—she was worried since the original problem started with pain in the right foot. She was using lavender heat bags, which she found helpful. She was having pilates lessons as well. Treatment: Using regular needles left KI-10, LU-5, and right SP-3 were supplemented. Light needling was applied to lower abdomen and supraclavicular fossa regions. Okyu/direct moxa was applied to GV-12 and BL-23. Summary: She came for periodic treatment for another 16 months. During this time she had no setbacks and returned to normal activities, including physical education and swimming. She had more stamina, was able to stand for longer, but still had some digestive issues.
 Put aside your own insecurity in the face of such problems and remember that it is most likely that this child will not improve if left untreated. Therefore, trying a few treatments to see if anything seems to change is a not unrealistic investment for the parent.
Put aside your own insecurity in the face of such problems and remember that it is most likely that this child will not improve if left untreated. Therefore, trying a few treatments to see if anything seems to change is a not unrealistic investment for the parent.
 Making a realistic assessment of what is possible and informing the parent of that—for example, stating to the parent of an autistic child that you cannot cure the autism, but you will try treatments that you and they may apply, to see if you can make its manifestations easier to deal with. In this case, you are giving the parents tools for helping daily life with their child. You are not only trying to help the child have fewer symptoms, but you are also helping the parent develop more caring and management skills; you are not trying to “cure” the child.
Making a realistic assessment of what is possible and informing the parent of that—for example, stating to the parent of an autistic child that you cannot cure the autism, but you will try treatments that you and they may apply, to see if you can make its manifestations easier to deal with. In this case, you are giving the parents tools for helping daily life with their child. You are not only trying to help the child have fewer symptoms, but you are also helping the parent develop more caring and management skills; you are not trying to “cure” the child.
 Think about an adjusted cost of treatment for the parents as they will be likely to need to come back over the long term once you have agreed that that is worthwhile trying.
Think about an adjusted cost of treatment for the parents as they will be likely to need to come back over the long term once you have agreed that that is worthwhile trying.
 Trust the judgments of the parent with regard to assessing how the child is doing. When you see a child only once a week and do not have to participate in their daily care, it can be difficult for you to see improvements. Sometimes the parent is very happy because certain seemingly small activities each day have improved. You would not have obtained information about these things in your normal course of questioning, and thus would not have been able to notice any improvements. An example of this might be an autistic child trying to socialize more with the other children and play more with them at the special daytime child care center (something they never did before) or trying to verbalize more to the parent.
Trust the judgments of the parent with regard to assessing how the child is doing. When you see a child only once a week and do not have to participate in their daily care, it can be difficult for you to see improvements. Sometimes the parent is very happy because certain seemingly small activities each day have improved. You would not have obtained information about these things in your normal course of questioning, and thus would not have been able to notice any improvements. An example of this might be an autistic child trying to socialize more with the other children and play more with them at the special daytime child care center (something they never did before) or trying to verbalize more to the parent.
The Lung Weak Constitution Patient
 Recurrent infections affecting the lungs (colds, “flu,” bronchitis, pneumonia), triggering recurrent infections in the nose and/or ears
Recurrent infections affecting the lungs (colds, “flu,” bronchitis, pneumonia), triggering recurrent infections in the nose and/or ears
 Chronic respiratory problems such as asthma, croup (in infants and younger children)
Chronic respiratory problems such as asthma, croup (in infants and younger children)
 Chronic skin problems such as eczema, atopic dermatitis
Chronic skin problems such as eczema, atopic dermatitis
 Severe, often multiple, contact or airborne allergies (“allergic constitution”)
Severe, often multiple, contact or airborne allergies (“allergic constitution”)
 The skin is often thin and feels more fragile. Sometimes veins are more clearly visible under the skin, such as on the chest and cheeks
The skin is often thin and feels more fragile. Sometimes veins are more clearly visible under the skin, such as on the chest and cheeks
The Spleen Weak Constitution Patient
 Chronic weakness of the digestive system, often with chronic loose stools or diarrhea
Chronic weakness of the digestive system, often with chronic loose stools or diarrhea
 Poor appetite, and in the infant severe problems with regurgitation, vomiting
Poor appetite, and in the infant severe problems with regurgitation, vomiting
 Severe, often multiple, food allergies (“allergic constitution”)
Severe, often multiple, food allergies (“allergic constitution”)
 Problems with weight gain, i.e., the “failure to thrive” child that falls below the normal growth (weight/height) curve; this child is often skinny, fatigued, and less active
Problems with weight gain, i.e., the “failure to thrive” child that falls below the normal growth (weight/height) curve; this child is often skinny, fatigued, and less active
The Kidney Weak Constitution Patient
 Autism, mental development or retardation problems
Autism, mental development or retardation problems
 Structural, locomotor problems, balance/gait problems
Structural, locomotor problems, balance/gait problems
 Paralysis or inability to use the limbs
Paralysis or inability to use the limbs
 Major organ dysfunctions or non-functioning organs (such as no bladder control)
Major organ dysfunctions or non-functioning organs (such as no bladder control)
The Liver Weak Constitution Patient
 Severe sleep disturbance
Severe sleep disturbance
 Severe irritability, crying, temper tantrums
Severe irritability, crying, temper tantrums
 Severe behavioral problems
Severe behavioral problems
 Stiff muscles most commonly over the neck, shoulders, upper and mid-back
Stiff muscles most commonly over the neck, shoulders, upper and mid-back
 Pain in the muscles due to poor adaptation and strain following growth spurts.
Pain in the muscles due to poor adaptation and strain following growth spurts.
General Approach for Patients with Weak Constitution
Goals of Treatment
Root Treatment for the Lung Weak Constitution Type
Core Non-pattern-based Root Treatment
Lung Vacuity Pattern Treatment
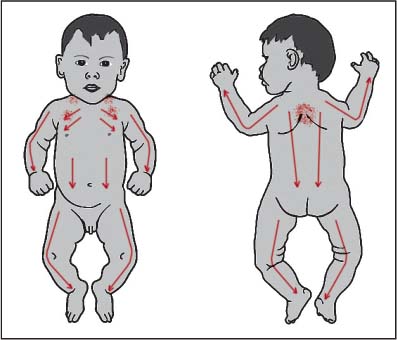
Additional Treatment
Root Treatment for the Spleen Weak Constitution Type
Core Non-pattern-based Root Treatment
Spleen Vacuity Pattern Treatment
Additional Treatment
Root Treatment for the Kidney Weak Constitution Type
Core Non-pattern-based Root Treatment
Kidney Vacuity Pattern Treatment
Additional Treatment
Root Treatment for the Liver Weak Constitution Type
Core Non-pattern-based Root Treatment
Liver Vacuity Pattern Treatment
Additional Treatment
 Lung weak constitution—Chapters 18, 19, 21, 26, 27
Lung weak constitution—Chapters 18, 19, 21, 26, 27
 Spleen weak constitution—Chapters 20, 21
Spleen weak constitution—Chapters 20, 21
 Kidney weak constitution—Chapter 24
Kidney weak constitution—Chapter 24
 Liver weak constitution—Chapter 21
Liver weak constitution—Chapter 21
Additional General Recommendations for Treatment of Weak Constitution
Further Case Histories
Naomi, Girl Age 10 Years
Weak Constitution
 Treatment is often needed over a long period of time, hence recommending home therapy can be a big advantage.
Treatment is often needed over a long period of time, hence recommending home therapy can be a big advantage.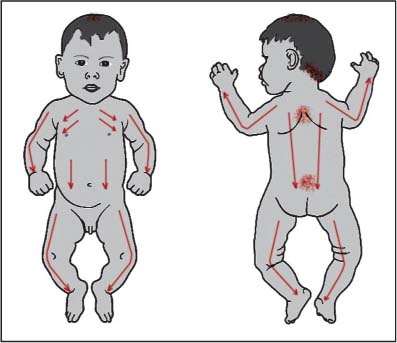
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


