28 Vasculitis
Etiology and Pathogenesis
Classification
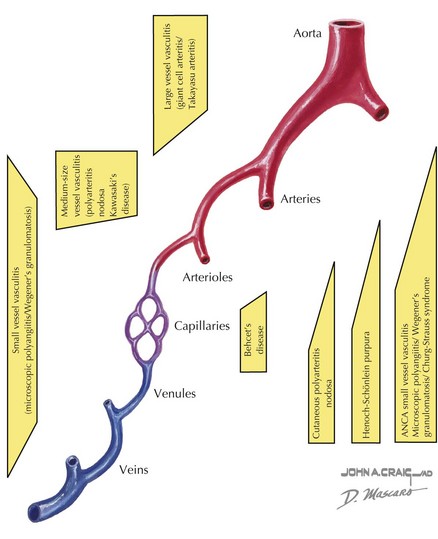
Vasculitis can be classified based on the involvement of primarily large, medium, or small vessels (Figure 28-1). In addition, certain vasculitides have a predilection for arteries, veins, or both. The vasculitides can be further classified as granulomatous or nongranulomatous. The granulomatous diseases include Takayasu arteritis, Wegener’s granulomatosis, and Churg-Strauss syndrome (see Chapter 30). The nongranulomatous vasculitides include PAN, KD, microscopic polyangiitis, HSP, cutaneous leukocytoclastic vasculitis, and essential cryoglobulinemic vasculitis.
Clinical Presentation
Certain patterns of clinical symptoms and organ involvement may be suggestive of a specific vasculitis (Box 28-1). For example, whereas palpable purpura, arthralgias, abdominal pain, and renal disease suggest HSP, persistent fever, conjunctivitis, cervical lymphadenopathy, extremity swelling, mucocutaneous changes, and rash suggest KD (see below). Microscopic polyangiitis is associated with high titers of pANCA (protoplasmic-staining antineutrophil cytoplasmic antibodies) and affects mainly the pulmonary and renal systems. Hypersensitivity vasculitis is a necrotizing vasculitis that presents with a papular rash that may be red or blistering and is often associated with infection or medication exposure. Hypocomplementemic urticarial vasculitis presents with urticarial skin lesions and low serum complement levels of C4 and C3. Behçet’s disease is a unique systemic vasculitis that affects both arteries and veins. The classic triad of Behçet’s disease includes oral ulcers, uveitis, and genital ulcers; however, any organ system can be affected.
PAN is a necrotizing vasculitis affecting the medium-sized arteries and can present with systemic disease or in a limited form that only involves the skin and joints. It occurs in school-aged children, and there is typically a history of a preceding upper respiratory infection or streptococcal pharyngitis. In unvaccinated children, hepatitis B can be causative. Symptoms include prolonged fevers, malaise, calf pain, testicular pain, and weight loss. Physical examination findings include painful nodules (particularly on the feet), livedo reticularis (see Figure 29-2), myalgias, and arthritis of large joints. In the systemic form, any organ system can be affected; thus, hypertension, renal abnormalities, gastrointestinal involvement, and coronary disease can be seen. Of the large vessel diseases, temporal arteritis is not seen in childhood. Takayasu arteritis, the third most common childhood vasculitis, preferentially affects the large branches of the aorta. Examination may reveal bruits, hypertension, and absent pulses.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


