CHAPTER 1 Vascular Access
Step 1: Surgical Anatomy
♦ The six central veins include the internal jugular, subclavian, and femoral veins. In most children, these are symmetric and paired.
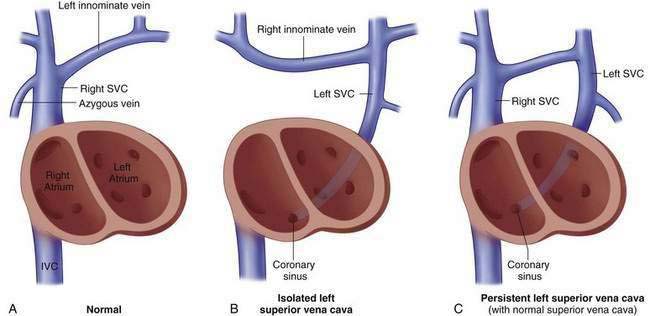
♦ Children with congenital heart disease, splenia syndromes, and variants of esophageal atresia have an increased incidence of anatomic variants in the subclavian veins that are relevant to central access procedures (Fig. 1-1).
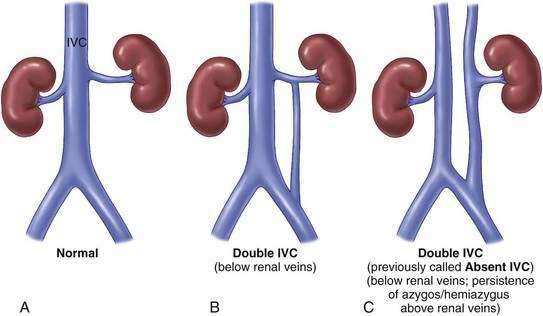
♦ Children with congenital heart disease and situs abnormalities have an increased incidence of variants of the inferior vena cava that are relevant (Fig. 1-2).
Step 2: Preoperative Considerations
♦ Does the patient have clinical indicators of coagulopathy or receive any medications that impact coagulation status?
Step 3: Operative Steps
1 General Concepts
♦ In general, insertion of most central lines in children is best achieved in the operating room with the patient under anesthesia and using fluoroscopy. It is not uncommon, however, to be asked to provide a central line in the emergency room or intensive care unit for an unstable patient who requires immediate access and is not stable enough for transport.
♦ In these patients, the use of bedside Doppler examination or ultrasound may be helpful in assessing position and patency of veins. This is particularly useful in children who have had multiple previous central lines. With Doppler probe, a good venous signal that varies with respiration suggests patency of the jugular and femoral systems, and the path of the signal may be mapped out using a skin marker. Good augmentation of the venous signal with compression of the leg also suggests patency of the femoral system.
♦ Bedside ultrasound may also demonstrate a patent vein that can be mapped using a skin marker or observed directly during venipuncture if a sterile probe is available.
♦ Operative records should be reviewed for information regarding previous placement of central lines.
♦ Regardless of the method or site of placement, a confirming radiographic image of the final result should be obtained.
2 Temporary Central Lines
♦ Temporary lines are inserted by percutaneous Seldinger technique directly into the vein and are generally acceptable for 2 to 3 weeks.
♦ The vein is accessed percutaneously using a thin-walled needle. After aspiration of nonpulsatile venous blood, the wire is advanced well into the vein.
♦ If venous blood is obtained, but the wire does not advance easily and fluoroscopy is available, contrast solution may be injected either through the needle or after replacing the needle over the wire with an angiocatheter and confirming continued ability to aspirate blood. This may demonstrate previously unrecognized thrombosis or congenital anatomic variants. If fluoroscopy is not available, repeat venipuncture, or an alternative site is needed.
♦ Once the wire has easily passed, the dilator is placed over the wire just deep enough to allow the tip of the dilator to pass through the skin and soft tissues. The wire should remain inserted well beyond the tip of the dilator.
3 Tunneled Central Lines
♦ The entry site is enlarged enough to allow the catheter tubing to be brought from a separate exit site.
♦ The exit site should be chosen several centimeters away in a location that will create a smooth pathway and a convenient place for the dressing.
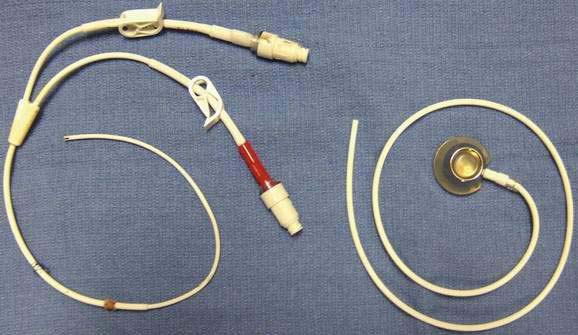
♦ The catheter may be either pulled through the tunnel antegrade with a blunt probe or pushed through the lumen of a Frazier tip sucker that is passed retrograde down the tunnel (Fig. 1-4).
♦ The cuff is positioned 1 cm above the exit site to allow for later removal without the need for additional incision.
♦ For percutaneous access, the peelaway or obturator sheath is advanced over the wire with fluoroscopic assistance (Fig. 1-5).
♦ The sheath is peeled away, and fluoroscopy is used again to confirm the proper course and position of the catheter (Fig. 1-7).
♦ A single nonabsorbable monofilament suture is used to secure the catheter at the exit site after confirming ability to aspirate and flush all lumens.
♦ For subcutaneous reservoirs, the reservoir should be placed in a flat location and secured to the fascia.