4 Understanding the Illness Experience and Providing Anticipatory Guidance
Matthew was a red-haired little boy suffering from congenital microvillus inclusion disease, an autosomal recessive disorder that is characterized by intestinal failure and often treated with multivisceral organ transplantation. This patient and his family experienced a great deal of suffering. When he was 5 years old, after a year-long hospitalization and careful consideration of prognosis and establishment of realistic goals of care, his family decided to bring him home despite concerns for the complexity of his care. He was discharged on multiple medications including continuous opioid infusion and parenteral nutrition under the care of the local hospice and palliative care team. Medical care continued at home as an integral aspect of a normal family life. His last months included a trip to a Nascar race, visits by a local fireman, and a full array of school services. Most importantly he was wrapped in the love of his two sisters, parents, and grandparents through his death (Figs. 4-1 to 4-3).




Establishing a Therapeutic Alliance
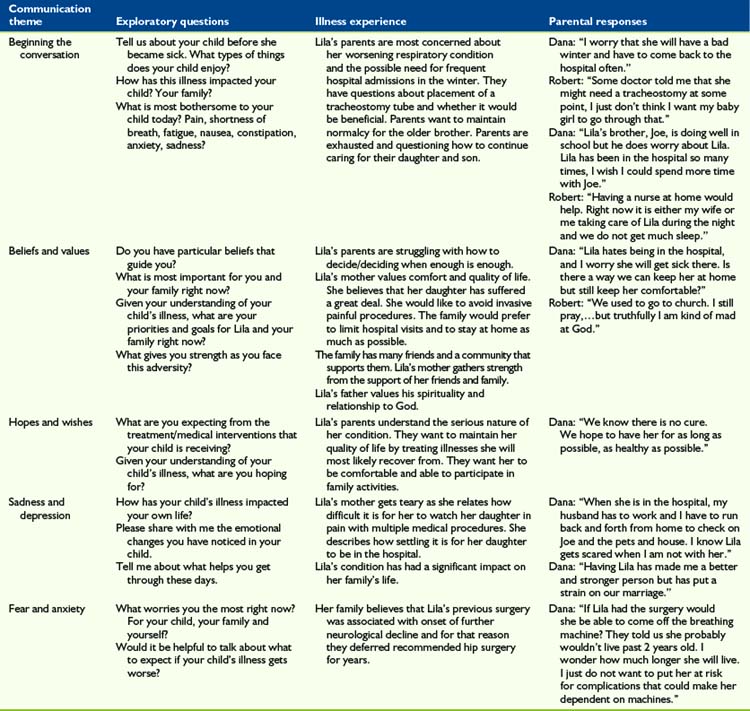
Understanding the patient’s and family’s beliefs, values, hopes, wishes, expectations, fears, and worries is crucial for clinicians who strive to create a plan of care with their patients. Clinicians must be willing to listen, empathize, solve problems, and encourage life-affirming events with patients and families as they face the challenges associated with a life-threatening illness. Misunderstandings and frustrations more often occur when clinicians offer treatment options without understanding the feelings, thoughts, and underlying themes that guide the patient’s and family’s decision-making process. A sample of exploratory responses that may be used in communicating with children and families is included in Table 4-1.
An essential part of establishing a therapeutic alliance is regular meetings with the patient and his or her family in which issues outlined in this chapter are discussed. Such discussions should be planned with care. For example, adequate time for in-depth conversation should be allotted, a private setting should be arranged, and the presence of both parents and/or others who are identified as primary supporters should be ensured. By listening respectfully and building on the parents’ knowledge, the interdisciplinary team (IDT)—which is typically composed of doctors, nurses, social workers, child life specialists, chaplains, and psychologists—can tailor information and educate the family about treatment options and other issues of relevance. Recommendations may be made based on the existing evidence, on realistic goals, and within the child’s and family’s psychosocial and spiritual context. Elements of anticipatory guidance in the palliative care setting are discussed in the following section and suggested themes are presented in Box 4-1.
Advanced Illness Care Planning
Ethical and Legal Considerations
Symptom Control
Care Coordination and Continuity
Understanding the Illness Experience
Beliefs and values
Beliefs and values give meaning to a person’s life. They influence the patient’s and family’s perceptions about how things are and how things should be. Values may dictate preferences in some circumstances. Patients with life-threatening conditions and their parents apply a set of values to guide decisions about medical care.1,2 Decisions made by patients and families about whether a certain treatment is desirable are often based on their determination of the treatment’s positive or negative qualities and whether it is perceived as beneficial. For those dealing with a progressive or incurable illness, these judgments may occur in the context of values that reflect the dual goal of seeking disease-directed therapies and comfort-directed care.3
Identifying and understanding the patient’s and family’s beliefs and values is an important palliative care skill that helps direct efforts toward improving the quality of end-of-life care. Having open and thoughtful conversations about the patient’s and family’s goals of care can be an effective approach to understanding their values and priorities. These conversations may also help patients and families who are not fully aware of the values they hold deeply and which may guide decisions about their care. In a study examining end-of-life care preferences, parents of seriously ill children identified the following as important end-of-life priorities: honest and complete information, ready access to staff, communication and care coordination, emotional expressions and support by staff, preservation of the integrity of the parent-child relationship, and faith.4 Moreover, when considering withdrawal of artificial life-sustaining support, parents placed the highest priorities on prognosis, quality of life, and their child’s level of comfort.5,6 Honoring these personal values may facilitate the family’s ability to maintain a sense of dignity and integrity.
An important universal value shared by seriously ill patients and their families is the presence of consistent and meaningful relationships within the family unit and with the care team.7 Relationship-based value judgments consistently inform patients’ preferences and decision making.8 Sometimes the expressed values of patients and families differ from those of their healthcare providers. In a study to ascertain parents’ and physicians’ assessments of quality of end-of-life care for children dying from cancer, Mack et al, found that for parents, doctor-patient communication is the principal determinant of high-quality physician care.9 Communicating with honesty and sensitivity about what to expect at the end of their child’s life, communicating directly with the child when appropriate, and preparing the parent for circumstances surrounding the child’s death were all cited by parents as high-quality care. In contrast, physicians’ ratings of high-quality end-of-life care depended on biomedical variables such as less pain and fewer days in the hospital rather than relational parameters. Consequently, clinicians are advised to think about what they consider important in the care of a patient at the end of life and acknowledge the risk of imposing their own value system in the context of a therapeutic alliance with a patient and family facing end-of-life care issues.
Hopes and wishes
In talking with patients and their families about hope, it is important for clinicians to distinguish being hopeful from wishful thinking, having unrealistic expectations, or feeling optimistic.10 Palliative care clinicians can help patients, families, and their healthcare providers by listening without judgment to their experiences and helping to solidify a deeper understanding of these concepts as they evolve in the context of serious illness. Ultimately, hope influences the decisions made by patients and families facing a life-threatening illness.
It is not uncommon to hear staff members worry that parents are not “getting it,” have not been told about the child’s prognosis, or are in denial when the parents make hopeful, optimistic, or wishful statements. A communication schism may occur, and the therapeutic alliance can be severely compromised, if parents are denied the opportunity to express their hopes and wishes. Patients and families may express their hopes and wishes interchangeably, and many use the language of hope in a religious or spiritual context. In the presence of progressive illness, hope can be a powerful coping mechanism, and caregivers must be careful not to strip it away through careless confrontation or premature conversations. It is difficult, however, to differentiate between expressions of wishful thinking and those of hope, and in practice, patients and families often experience a combination of the two. Although helping the patient or family to reframe hope may be appropriate in some circumstances, clinicians must do so only in the context of a relationship based on trust and always remain respectful of the patient’s and family’s overall experiences. A clinician’s responsibility is to acknowledge hope and gently reframe the patient’s and family’s expectations by providing relevant clinical data. In a study to evaluate the relationship between prognostic disclosure and hope, Mack et al. found that parents who received more information about the patient’s prognosis and had high-quality communication were more likely to report communication-related hope, even when the likelihood of a cure was low.11 Such conversations may allow for a balanced perspective of hope for cure and expectations of benefit from treatment.
Sadness and depression
Expressions of hopelessness are often accompanied by profound sadness, defined as an emotional state of varying intensity characterized by feelings of unhappiness.12 Sadness, sorrow, or desolation are normal responses when individuals face a threat to meaningful relationships, a loss of their personal values, or feelings of loneliness and isolation. Sadness in children may be their mourning the loss of the life they previously had (e.g., interacting with friends, playing, attending school) as well as their threatened future; parents mourn the loss of the dreams they held for their child.
Learning to distinguish between sadness and depression is important in palliative care. Depression is a mood disorder characterized by the loss of self-esteem, feelings of guilt, anger, and despair, and negative views about one’s own future. A profound sense of hopelessness at times may be accompanied by suicidal ideation.10 Symptoms of depression include fatigue, insomnia, decreased performance at school or work, loss of appetite, loss of interest in activities previously enjoyed, and social withdrawal. In general, the source of sadness is more specific than that of depression, and a sad person is usually able to experience pleasure and happiness about other aspects of his or her life. For a depressed person, sadness and hopelessness are broader and more pervasive. Although encouraging patients and families to openly share their feelings and reconnect with loved ones may alleviate their sadness, concerns about depression may warrant a psychiatric consult, counseling, and pharmacotherapy.13,14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


