68 Thyroid Disease
Thyroid Hormone Production
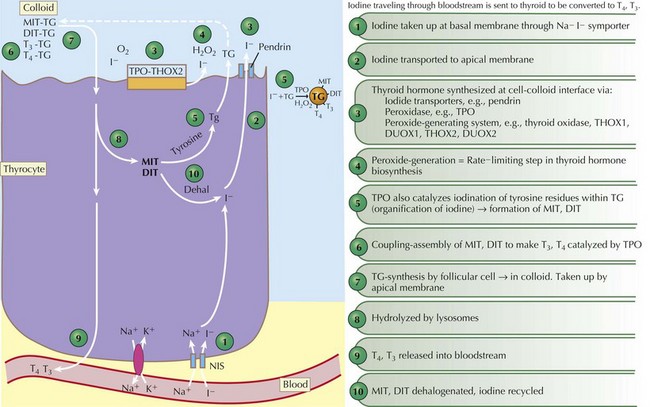
Thyroid hormones are produced by the coupling of iodine molecules to the amino acid tyrosine (Figure 68-1). The principal secreted thyroid hormone is T4. The normal thyroid secretes only small amounts of T3, and most circulating T3 (≈70%-90%) is derived from peripheral deiodination of T4. Thyroid hormones circulate bound to carrier proteins, including thyroid-binding globulin (TBG), transthyretin (thyroxine-binding prealbumin), and albumin. Less than 1% of circulating T4 and T3 are unbound or “free.”
Congenital Hypothyroidism
Etiology and Pathogenesis
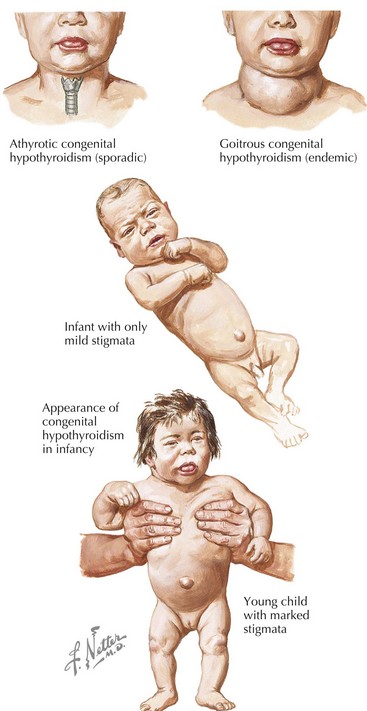
Congenital hypothyroidism (CH) is one of the most common causes of preventable mental retardation (Figure 68-2). Fortunately, early identification and rapid treatment lead to normal neurocognitive development. Although approximately 10% of cases of CH are transient and caused by factors such as iodine exposure, prematurity, or maternal transfer of antithyroid antibodies, in most cases, hypothyroidism is permanent. Worldwide, iodine deficiency is the most common cause of CH. However, in areas of the world where iodine deficiency is uncommon, CH most commonly results from thyroid dysgenesis (≈75% of cases); thyroid dyshormonogenesis (≈10%), TSH deficiency (5%), and genetic defects in the TSH receptor are much less common. The incidence of CH is approximately one in 3000 to 4000 births. In most cases, CH is sporadic, but mutations in genes encoding transcription factors that are required for normal development of the thyroid gland are present in about 10% to 15% of cases. Circulating levels of TSH are elevated and thyroid hormone levels are low in those with CH.
Evaluation (Figure 68-3)
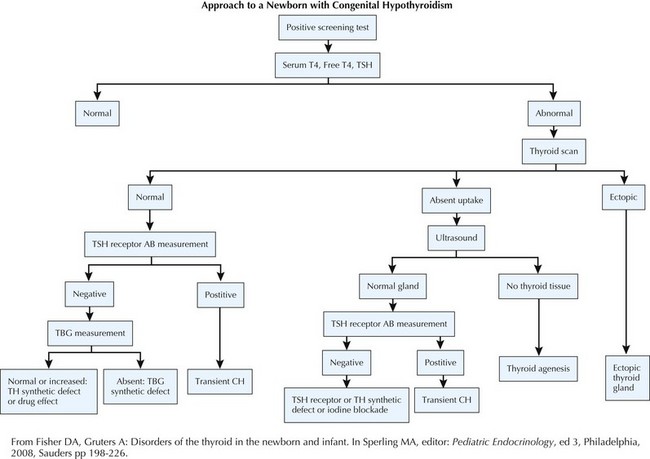
Figure 68-3 Evaluation of congenital hypothyroidism.
AB, antibody; CH, congenital hypothyroidism; TBG, thyroid-binding globulin; TH, thyroid hormone; TSH, thyroid-stimulating hormone.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


