CHAPTER 3 Thyroglossal Duct Cyst
Step 1: Surgical Anatomy
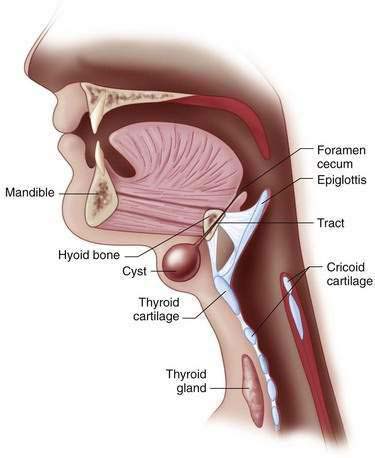
♦ Thyroglossal duct cyst traditionally manifests as a painless midline anterior cervical mass that often moves with swallowing (Fig. 3-1).
♦ The cyst occasionally communicates with the skin as a draining sinus, and its tract always extends through the center of the hyoid bone to terminate at the tongue base (Fig. 3-2). Operative extirpation of the entire cyst and sinus tract, including the involved portion of the hyoid bone, is critical to avoid a recurrence.
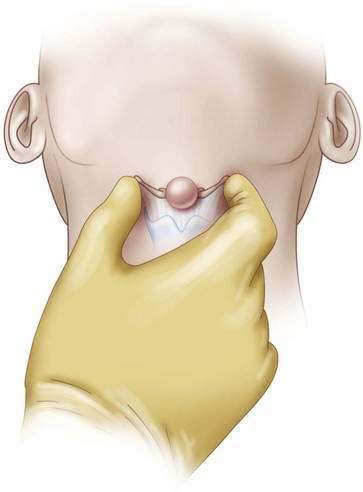
♦ The greater horns of the hyoid bone may be palpated bilaterally and moved side to side, which will result in cyst movement (Fig. 3-3) and help to ensure a proper anatomic resection and avoid injuring the larynx.

Step 2: Preoperative Considerations
♦ The diagnosis of thyroglossal duct cyst is made by a history and physical examination, although an ultrasound may help to differentiate this lesion from a dermoid cyst, epidermoid cyst, or median ectopic thyroid. An extensive radiographic and laboratory evaluation is unnecessary.
♦ Surgical excision is indicated on identification and is easiest in the absence of infection. Most infections can be treated with oral antibiotics targeting Haemophilus influenzae, Staphylococcus aureus, and Staphylococcus epidermidis, but occasionally the abscess is medically refractory and requires drainage. Elective resection is then best reserved for a time when the wound has healed and the inflammation is minimized.
Step 3: Operative Steps
Anesthetic Induction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


