Chapter 24 The Adolescent Well Visit
Medical Knowledge and Patient Care
Background and Adolescent Morbidity
Whereas congenital anomalies and malignant neoplasms are the leading causes of death in childhood, high-risk behaviors manifest during adolescence and place the individual at risk for related morbidities and even mortality.1,2 In the United States, unintentional injury, homicide, and suicide are leading causes of death among 15- to 19-year-olds. Seventy-one percent of all deaths among persons 10 to 24 years of age result from four causes: motor vehicle crashes, other unintentional injuries, homicide, and suicide.2 The 2005 Youth Risk Behavior Survey conducted by the Centers for Disease Control and Prevention showed that 10% of high school students had driven a car or other vehicle when they had been drinking alcohol, and close to 20% had carried a weapon. Thirty-six percent of high school students had been in a physical fight during the 12 months preceding the survey, and 8% had attempted suicide.
Psychosocial Problems
Nearly 50% of those surveyed admitted to having had sexual intercourse, and 37% did not use a condom during their most recent sexual intercourse. Half of respondents admitted to drinking alcohol frequently, 20% had used marijuana, and 2% had injected illegal drugs. Feeling sad or hopeless is also common among adolescents. The survey found that during the preceding 12 months, 28.5% of the teens surveyed had felt so sad or hopeless almost every day for 2 or more weeks in a row that they stopped doing some usual activities.2 Another study found that 4.6% of those 13 to 17 years of age were taking medications to treat attention-deficit/hyperactivity disorder (ADHD), with 16-year-old males having the highest prevalence of 14.9%.3
The two major causes of death in adults, cardiovascular disease and cancer, may in fact have their origins in adolescence, and possibly childhood. During 2005, 25% of high school students had admitted to smoking cigarettes during the 30 days preceding the Youth Risk Behavior Survey. Sixty-seven percent did not attend regular physical education classes, and 13% were overweight.2
Phases of Adolescence
Adolescence, a period of tremendous physical growth, is divided into three phases: early (11 to 14 years), middle (15 to 17 years), and late adolescence (18 to 21 years). Weight gain during puberty accounts for about 50% of ideal adult weight, and linear growth during puberty accounts for 20% to 25% of adult height. Up to two-thirds of adult bone mass is accrued during this period. It is also a time of marked divergence in the physical features and body habitus of females versus males that goes beyond gonadal and breast development. Female body fat increases from about 16% to about 27%. When puberty is complete, males have 50% more lean body mass than women, and women have twice the body fat of men. Ninety-five percent of females complete growth by age 16, whereas 95% of males complete growth by age 18.4
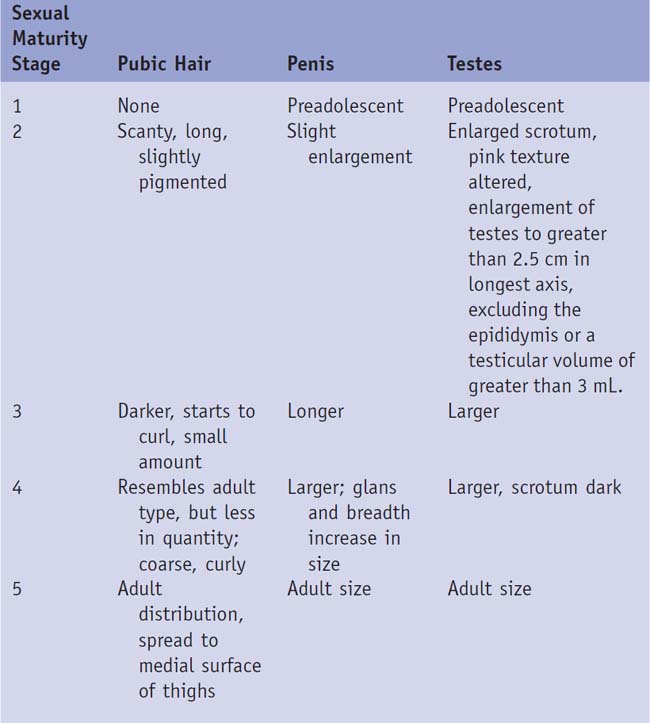
Menarche occurs and pubertal development goes through predictable stages as outlined in Table 24-1 for girls and Table 24-2 for boys and Figures 24-1 and 24-2.
Table 24-1 Classification of Sexual Maturity Stages in Girls
| Sexual Maturity Stage | Pubic Hair | Breasts |
|---|---|---|
| 1 | Preadolescent | Preadolescent |
| 2 | Sparse, lightly pigmented, straight, medial border of labia | Breast and papilla elevated as small mound; areolar diameter increased |
| 3 | Darker, beginning to curl, increased amount | Breast and areola enlarged, no contour separation |
| 4 | Coarse, curly, abundant but amount less than in adult | Areola and papilla form secondary mound |
| 5 | Adult feminine triangle, spread to medial surfaces of thighs | Mature; nipple projects, areola part of general breast contour |
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


