5 The Acute Abdomen
Etiology and Pathogenesis
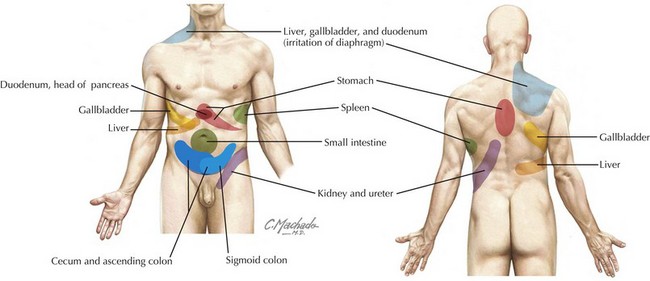
Referred pain is often perceived at sites distant from the affected organ and may be described either as sharp and localized or as a vague aching sensation (Figure 5-1). Examples include irritation of the parietal pleura of the lung perceived as abdominal wall pain and inflammation of the gallbladder perceived as scapular pain.
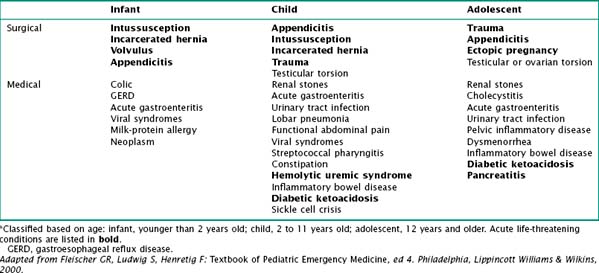
It is helpful to classify the cause of acute abdominal pain by age (Table 5-1). There are many potential causes of abdominal pain, including infectious, anatomic, traumatic, inflammatory, functional, and oncologic.
Clinical Presentation
Differential Diagnosis
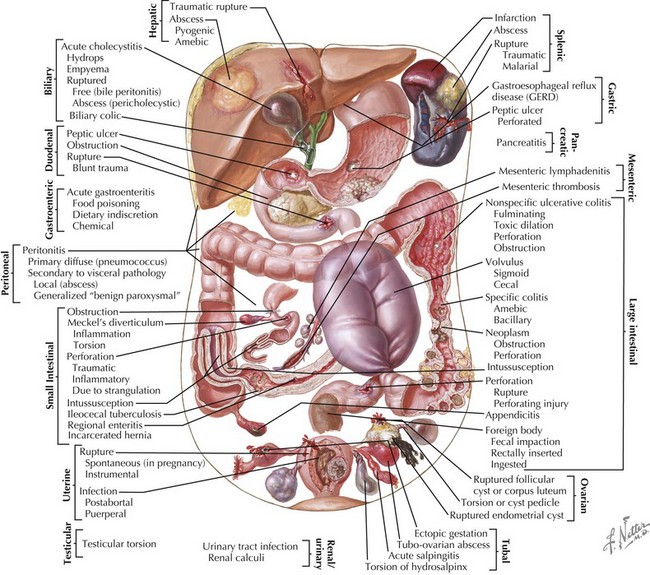
The differential diagnosis for abdominal pain in children is very broad, and it can be approached in different ways (Figure 5-2). Certain conditions occur more commonly at specific ages and therefore it may be useful to classify causes of acute abdominal pain based on age. Pain may also be classified as surgical or medical (Table 5-1).
Across all ages, gastroenteritis and appendicitis are the most common medical and surgical causes of acute abdominal pain, respectively. Malrotation with midgut volvulus is the single most devastating abdominal surgical emergency of childhood (see Chapter 109).
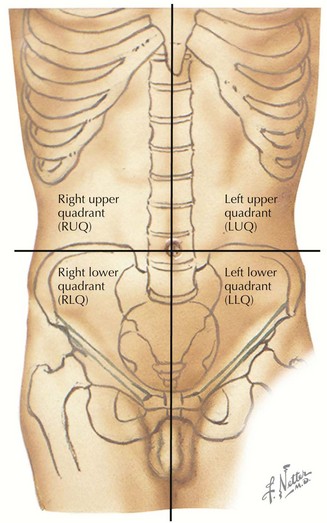
Abdominal pain can also be classified based on the location of the pain. A classic approach is by dividing the abdomen into four quadrants (Figure 5-3). This can help the practitioner direct the workup to rule in or out the most common diagnoses based on the location of symptoms. For example, hepatic and gallbladder disease usually present with right upper quadrant pain (see Chapter 115). Appendicitis classically presents with migration of pain to the RLQ. Gastritis or peptic ulcer disease may present with left upper quadrant pain (see Chapter 108).
Pain Character
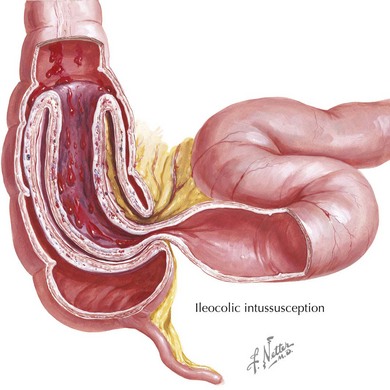
Infants and young children can seldom localize their pain, and parents often describe an inconsolable child who lies with his or her legs drawn up to the chest. Asking the parents if they think the child is in pain can be helpful to distinguish pain from fussiness or irritability. Pain that is intermittent, with paroxysms of cramping inconsolable pain alternating with return to normal state, is characteristic of intussusception (Figure 5-4). Peritoneal irritation is suggested by pain that is worse with movements that change the tension of the abdominal wall, such as a bumpy car ride or walking. Pain that improves after vomiting or a bowel movement reflects a small bowel or large bowel cause, respectively.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


