CHAPTER 32 Testicular Torsion
Step 1: Surgical Anatomy
♦ Acute scrotal pain, particularly with erythema and edema, is the usual presentation of testicular torsion. The differential diagnoses of the acute scrotum are numerous (see Table 32-1), but testicular torsion, which results from a twisting of the spermatic cord, is the most serious and is a true surgical emergency.
♦ In the non-neonate, the physical examination findings are typically characterized by a unilaterally tender scrotum with varying degrees of erythema and edema. The testicle tends to ride higher in the scrotum and have a characteristic transverse orientation (Fig. 32-1).
♦ An anatomic anomaly of incomplete testicular fixation or “bell-clapper” deformity is necessary for testicular torsion to occur in the non-neonate (Fig. 32-2). This type of torsion is termed intravaginal, with the twist occurring within the tunica vaginalis because of the lack of normal attachments of the tunica vaginalis along the posterior aspect of the cord, epididymis, and testicle (Fig. 32-3).
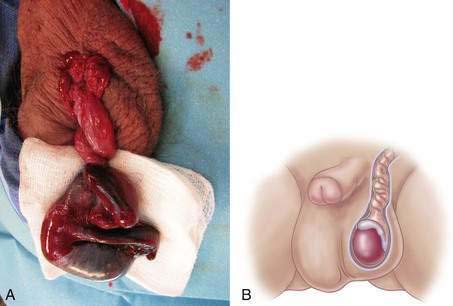
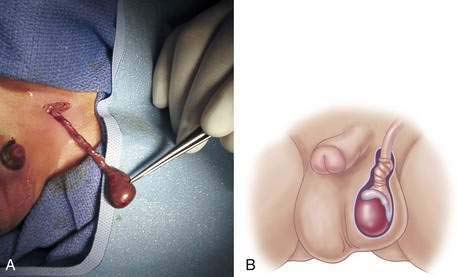
♦ In the neonate, the twist usually occurs proximal to the tunica vaginalis in the perinatal period, before the normal investment of the tunica vaginalis to the scrotum, which usually occurs by about 6 weeks of life (Fig. 32-4).
Table 32-1 Acute Scrotal Pain—Differential Diagnoses


Step 2: Preoperative Considerations
♦ In the neonate, the classic examination shows a dark, firm hemiscrotum with or without obvious tenderness and erythema, depending on when the torsion occurs perinatally (Fig. 32-5). In the older child, the hemiscrotum is usually significantly tender and erythematous as described above. The classic history is the sudden onset of unilateral testicular pain that is unrelenting and often associated with nausea and vomiting.
♦ A “golden” period of 4 to 8 hours from the time of torsion is considered the acceptable time frame to operate in order to have the best chance for testicular salvage. In the neonate, that period may be long past the time the patient delivers, and the chance of testicular salvage is typically not good.
♦ In the older child, time is of the essence, and every effort should be made to get to the operating room as soon as possible if the patient has a history and examination consistent with torsion.
♦ Other diagnostic studies most often are indicated in the patient with a nonclassic history or examination. Radioisotope scanning has been used historically to determine testicular flow, but it has mostly been replaced with high-resolution ultrasound with color-flow Doppler.



