CHAPTER 11 Surgical Treatment of Chest Wall Deformities
Nuss Procedure
Step 1: Surgical Anatomy
♦ Pectus excavatum is the most common chest wall deformity in children. Its incidence is estimated at approximately 1 in 100 children, and it has a male-to-female ratio of 3-4:1.
♦ Morphologic distinctions in pectus excavatum simplify the diagnosis and aid in the surgical correction. The deformities may be small in diameter and deep, “cup-shaped” or of large diameter and shallow, “saucer-shaped,” or eccentric.
Step 2: Preoperative Considerations
♦ A complete history and physical examination are performed on all patients. All patients are encouraged to perform exercises designed to strengthen the chest and back muscles and improve exercise tolerance, along with maintaining proper posture.
♦ Determination of a severe pectus excavatum and the need for repair includes two or more of the following criteria:




♦ Our experience has shown that the optimal age for repair is 10 to 14 years because patients’ chests are still soft and malleable. At this age, they show quick recovery, a rapid return to normal activities, and excellent results. After puberty, the flexibility of the chest wall is decreased and often requires the insertion of two bars. It also takes the patients longer to recover at this age. However, we have performed the procedure in patients up to age 31 years with good results.
Step 3: Operative Steps
Anesthetic Induction
♦ Standard endotracheal anesthesia is used for surgical correction, and epidural analgesia is used both as an adjunct during surgery and continued for pain control for an average of 3 days postoperatively.
Before Incision
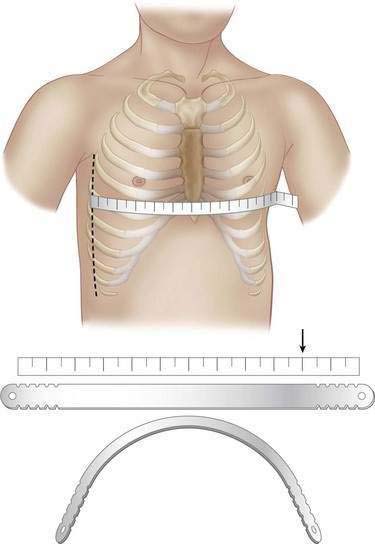
♦ The length of the pectus bar is determined by measuring the distance from the right midaxillary line to the left midaxillary line and subtracting 2 cm or 1 inch. The measurement is done over the area of the deepest depression that is still part of the sternum.
♦ The bar is bent to the desired convex configuration, making note that the center of the bar should have a negligible bend to allow greater stability (Fig. 11-1).