Chapter 367 Sudden Infant Death Syndrome
The sudden, unexpected death of an infant that is unexplained by a thorough postmortem examination, which includes a complete autopsy, investigation of the scene of death, and review of the medical history, constitutes sudden infant death syndrome (SIDS). An autopsy is essential to identify possible natural explanations for sudden, unexpected death such as congenital anomalies or infection and to diagnose traumatic child abuse (Tables 367-1, 367-2, 367-3). The autopsy typically cannot distinguish between SIDS and intentional suffocation, but the scene investigation and medical history may be of help if inconsistencies are evident.
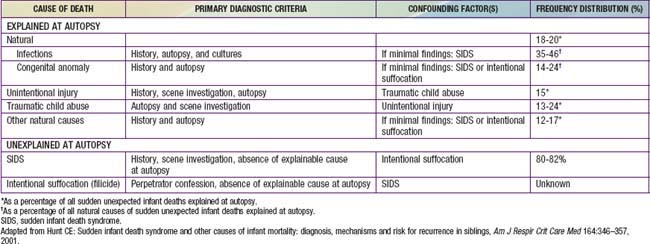
Table 367-2 CONDITIONS THAT CAN CAUSE APPARENT LIFE-THREATENING EVENTS OR SUDDEN DEATH
CENTRAL NERVOUS SYSTEM
CARDIAC
PULMONARY
GASTROINTESTINAL
ENDOCRINE-METABOLIC
INFECTION
TRAUMA
POISONING
From Kliegman RM, Greenbaum LA, Lye PS: Practical strategies in pediatric diagnosis and therapy, ed 2, Philadelphia, 2004, Elsevier Saunders, p 98.
Table 367-3 DIFFERENTIAL DIAGNOSIS OF RECURRENT SUDDEN INFANT DEATH IN A SIBSHIP
IDIOPATHIC
Recurrent true sudden infant death syndrome
CENTRAL NERVOUS SYSTEM
CARDIAC
PULMONARY
Pulmonary hypertension
ENDOCRINE-METABOLIC
See Table 367-2
INFECTION
Disorders of immune host defense
CHILD ABUSE
From Kliegman RM, Greenbaum LA, Lye PS: Practical strategies in pediatric diagnosis and therapy, ed 2, Philadelphia, 2004, Elsevier Saunders, p 101.
Pathology
SIDS victims have several identifiable changes in the lungs and other organs and in brainstem structure and function. Nearly 65% of SIDS victims have structural evidence of pre-existing, chronic low-grade asphyxia, and other studies have identified biochemical markers of asphyxia. SIDS victims have higher levels of vascular endothelial growth factor (VEGF) in the cerebrospinal fluid (CSF). These increases may be related to VEGF polymorphisms (see Genetic Risk Factors) or might indicate recent hypoxemic events, because VEGF is upregulated by hypoxia. Brainstem findings include a persistent increase of dendritic spines and delayed maturation of synapses in the medullary respiratory centers, and decreased tyrosine hydroxylase immunoreactivity and catecholaminergic neurons. Decreases in serotonin 1A (5-HT1A) and 5-HT2A receptor immunoreactivity have been observed in the dorsal nucleus of the vagus, solitary nucleus, and ventrolateral medulla, whereas increases are present in periaqueductal gray matter of the midbrain. The decreased immunoreactivity of receptors is accompanied by brainstem gliosis, and it is therefore unclear whether the decreases are secondary to hypoxia or ischemia or whether they reflect primary alterations in 5-HT metabolism or transport (see Genetic Risk Factors) (Table 367-4).
Table 367-4 IDENTIFIED GENES FOR WHICH THE DISTRIBUTION OF POLYMORPHISMS DIFFERS IN SUDDEN INFANT DEATH SYNDROME INFANTS COMPARED TO CONTROL INFANTS
CARDIA CHANNELOPATHIES (7)
SEROTONIN (5-HT) (3)
GENES PERTINENT TO DEVELOPMENT OF AUTONOMIC NERVOUS SYSTEM (8)
INFECTION AND INFLAMMATION (6)
ENERGY PRODUCTION (1)
Mitochondrial DNA (mtDNA) polymorphisms
Adapted from Hunt CE, Hauck FR: Sudden infant death syndrome: gene-environment interactions. In Brugada R, Brugada J, Brugada P, editors: Clinical care in inherited cardiac syndromes, Guildford, UK, 2009, Springer-Verlag London.
Environmental Risk Factors
Declines of 50% or more in rates of SIDS in the USA and around the world have occurred in the past decade, at least in part as a result of national education campaigns directed at reducing risk factors associated with SIDS. The reductions in risk appear to be related primarily to decreases in placing infants prone for sleep and increases in placing them supine. A number of other risk factors also have significant associations with SIDS (Table 367-5); although many are nonmodifiable and most of the modifiable factors have not changed appreciably, self-reported maternal smoking prevalence during pregnancy has decreased by 25% in the past decade.
Table 367-5 ENVIRONMENTAL FACTORS ASSOCIATED WITH INCREASED RISK FOR SUDDEN INFANT DEATH SYNDROME
MATERNAL AND ANTENATAL RISK FACTORS
INFANT RISK FACTORS:



