Puerperal Tubal Sterilization
For several days after delivery, the uterine fundus lies at the level of the umbilicus, and fallopian tubes are accessible directly beneath the abdominal wall. Moreover, abdominal laxity allows easy repositioning of the incision over each uterine cornu. Thus, puerperal sterilization is technically simple, and hospitalization need not be prolonged.
Some prefer to perform sterilization immediately following delivery, although others wait for 12 to 24 hours. At Parkland Hospital, puerperal tubal ligation is performed in the obstetrical surgical suite the morning after delivery. This minimizes hospital stay but lowers the likelihood that postpartum hemorrhage would complicate recovery following surgery. In addition, the status of the newborn can be better ascertained before surgery.
Various techniques are now used to disrupt tubal patency. In general, a midtubal segment of fallopian tube is excised, and the severed ends seal by fibrosis and peritoneal regrowth. Commonly used methods of interval sterilization include the Parkland, Pomeroy, and modified Pomeroy techniques (American College of Obstetricians and Gynecologists, 2013). Irving and Uchida techniques or Kroener fimbriectomy are rarely used because they involve increased dissection, operative time, and chance of mesosalpingeal injury. With fimbriectomy, unfavorably high failure rates stem from recanalization of the proximal tubal segment (Pati, 2000).
Surgical Technique
If scheduled for the first postpartum day, puerperal sterilization is typically completed using spinal analgesia. If done more proximate to delivery, the same epidural catheter used for labor analgesia can be used for sterilization analgesia. General anesthesia may be less desirable due to residual pregnancy-related airway changes (Bucklin, 2003).
The bladder is emptied before surgery. A small infraumbilical incision is made. Adequate exposure is critical, and Army-Navy or appendiceal retractors are usually suitable. For obese women, a slightly larger incision and narrow Deaver retractors may be required. If bowel or omentum is obstructing, then Trendelenburg position may be helpful. Digitally packing with a single, moist, fanned-out piece of surgical gauze may also be used, but a hemostat should always be attached to the distal end to avert its retention. It is sometimes helpful to tilt the entire table to the opposite side of the tube being exposed.
The fallopian tube is identified and grasped at its midportion with a Babcock clamp, and the distal fimbria confirmed. This prevents confusing the round ligament with the midportion of the tube. A common reason for sterilization failure is ligation of the wrong structure, typically the round ligament. Therefore, identification and isolation of the distal tube prior to ligation is necessary. Whenever the tube is inadvertently dropped, it is mandatory to repeat this identification procedure. Surgical steps for ligation are outlined in Figures 39-1 and 39-2.
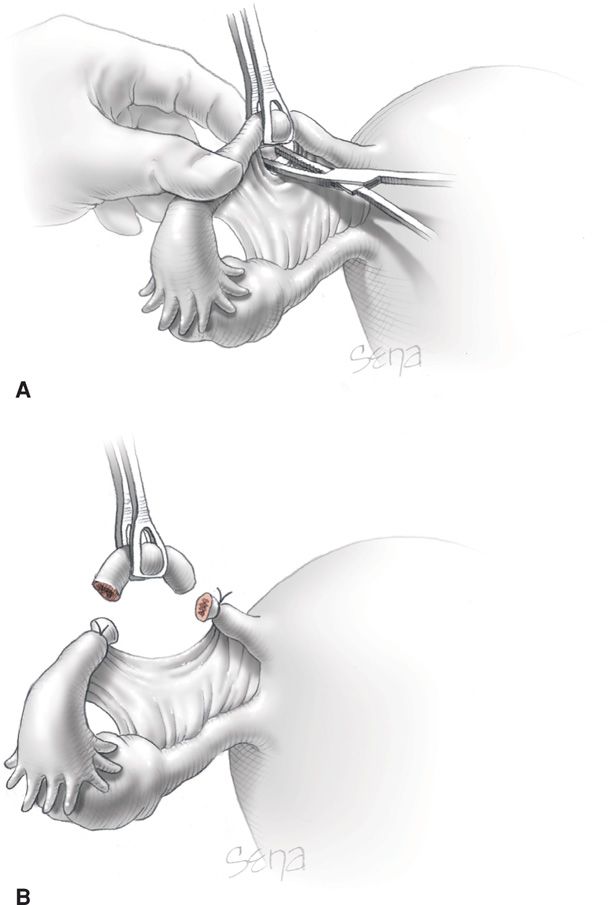
FIGURE 39-1 Parkland method. A. An avascular site in the mesosalpinx adjacent to the fallopian tube is perforated with a small hemostat. The jaws are opened to separate the fallopian tube from the adjacent mesosalpinx for approximately 2.5 cm. B. The freed fallopian tube is ligated proximally and distally with 0-chromic suture. The intervening segment of approximately 2 cm is excised, and the excision site is inspected for hemostasis. This method was designed to avoid the initial intimate proximity of the cut ends of the fallopian tube inherent with the Pomeroy procedure. (From Word, 2012, with permission.)
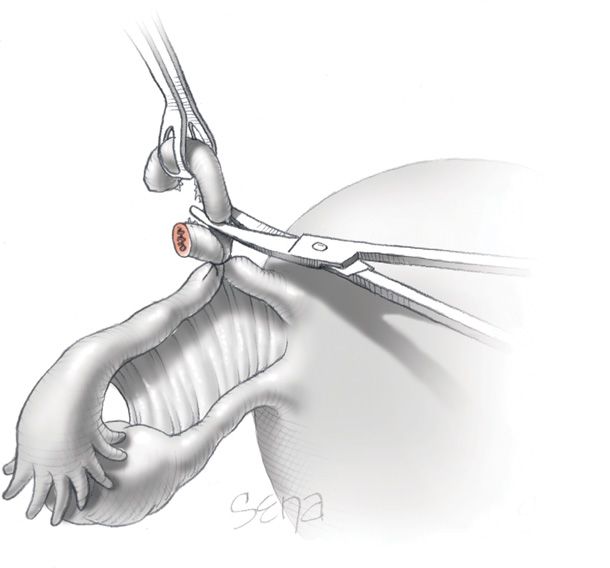
FIGURE 39-2 Pomeroy method. During ligation of a midsegment tubal loop, plain catgut is used to ensure prompt absorption of the ligature and subsequent separation of the severed tubal ends. (From Word, 2012, with permission.)
After surgery, diet is given as tolerated. Ileus is infrequent and should prompt concern for bowel injury, albeit rare. Most women have an uncomplicated course and are discharged on the first postoperative day.
 Nonpuerperal (Interval) Surgical Tubal Sterilization
Nonpuerperal (Interval) Surgical Tubal Sterilization
These techniques and other modifications basically consist of (1) ligation and resection at laparotomy as described earlier for puerperal sterilization; (2) application of permanent rings, clips, or inserts to the fallopian tubes by laparoscopy or hysteroscopy; or (3) electrocoagulation of a tubal segment, usually through a laparoscope. A detailed description and illustration of these can be found in Williams Gynecology, 2nd edition (Thompson, 2012).
In the United States, a laparoscopic approach to interval tubal sterilization is the most common. The procedure is frequently performed in an ambulatory surgical setting under general anesthesia. In almost all cases, the woman can be discharged within several hours. Minilaparotomy using a 3-cm suprapubic incision is also popular, especially in resource-poor countries (Kulier, 2004). Although not commonly used, the peritoneal cavity can be entered through the posterior vaginal fornix—colpotomy or culdotomy—to perform tubal interruption. Major morbidity is rare with either minilaparotomy or laparoscopy.
 Long-Term Complications
Long-Term Complications
Contraceptive Failure
Pregnancy following sterilization is uncommon. The Collaborative Review of Sterilization (CREST) study followed 10,863 women who had undergone tubal sterilization from 1978 through 1986 (Peterson, 1996). The cumulative failure rate for the various tubal procedures was 18.5 per 1000 or approximately 0.5 percent. The study found puerperal sterilization to be highly effective. The 5-year failure rate was 5 per 1000, and for 12 years, it was 7 per 1000.
Puerperal sterilization fails for two major reasons. First, surgical errors occur and include transection of the round ligament or only partial transection of the tube. For this reason, both tubal segments are submitted for pathological confirmation. Second, a fistulous tract or spontaneous reanastomosis may form between the severed tubal stumps.
Interval tubal sterilization may fail for several reasons. First, it may be due to equipment failure such as a defective current for electrosurgery or an insufficiently occlusive clip (Belot, 2008). Second, failure may result from fistula formation, especially with electrosurgical procedures, or the fallopian tube may undergo spontaneous reanastomosis. A third possibility is that the woman may have been already pregnant at the time of surgery—a so-called luteal phase pregnancy. To limit this possibility, surgery may ideally be performed during the follicular phase, and an effective contraceptive method used before surgery. Last, in some cases, no reason is found. Importantly, Soderstrom (1985) found that most sterilization failures were not preventable.
Approximately 30 percent of pregnancies that follow a failed tubal sterilization procedure are ectopic. This rate rises to 50 percent for those following a bipolar coagulation procedure (McCausland, 1980; Peterson, 1997). Thus, any symptoms of pregnancy in a woman after tubal sterilization must be investigated, and an ectopic pregnancy excluded.
Other Effects
Ovarian and breast cancer risks are either decreased or unaffected following sterilization (Ness, 2011; Press, 2011). Women who have undergone tubal sterilization are highly unlikely to subsequently have salpingitis (Levgur, 2000). An almost twofold increased incidence of functional ovarian cysts follows tubal sterilization (Holt, 2003). Several investigators have evaluated the risk of menorrhagia and intermenstrual bleeding following tubal sterilization, and most have found no association (DeStefano, 1985; Peterson, 2000; Shy, 1992).
Less objective but important psychological sequelae of sterilization have also been evaluated. In the CREST study, Costello (2002) found that tubal ligation did not change sexual interest or pleasure in 80 percent of women. In most of the 20 percent of women who did report a change, positive effects were 10 to 15 times more likely.
Invariably, a number of women express regrets regarding sterilization, and this is especially true if performed at a younger age (Curtis, 2006; Kelekçi, 2005). In the CREST study, Jamieson (2002) reported that 7 percent of women who had undergone tubal ligation had regrets by 5 years. This is not limited to their own sterilization, because 6.1 percent of women whose husbands had undergone vasectomy had similar regrets.
 Reversal of Tubal Sterilization
Reversal of Tubal Sterilization
No woman should undergo tubal sterilization believing that subsequent fertility is guaranteed by either surgery or by assisted reproductive techniques. Both approaches are technically difficult, expensive, and not always successful. Pregnancy rates following surgical reanastomosis are higher in younger women, in those with significant tubal length remaining, and in those with isthmic-to-isthmic repairs (American Society for Reproductive Medicine, 2012). With surgical reversals, pregnancy rates vary from 45 to 85 percent (Trussell, 2003; Van Voorhis, 2000). Almost 10 percent of women who became pregnant following reversal of tubal sterilization have an ectopic pregnancy.
 Salpingectomy and Hysterectomy
Salpingectomy and Hysterectomy
Newer evidence suggests that the fallopian tube may be the origin of pelvic serous carcinomas, especially those of the ovary. With this knowledge, the Society of Gynecologic Oncologists (2013) has issued a practice statement recommending salpingectomy to lower cancer risks. Specifically, for women at average risk of ovarian cancer, risk-reducing salpingectomy should be discussed and considered with patients at the time of abdominal or pelvic surgery, with hysterectomy, or in lieu of tubal ligation. Initial steps of salpingectomy are shown in Figure 39–3. Further illustration and discussion of surgical steps are outlined in Williams Gynecology, 2nd edition (Word, 2012).
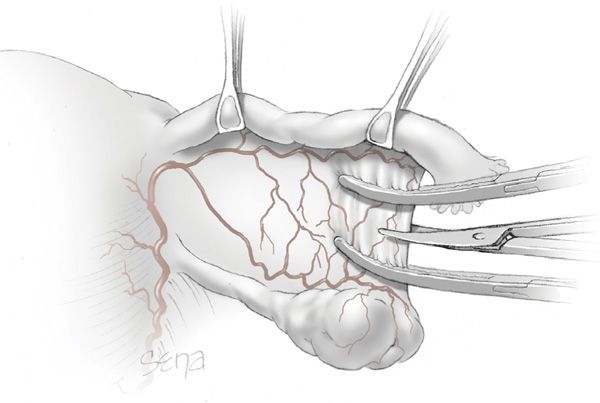
FIGURE 39-3 With salpingectomy, the mesosalpinx is sequentially clamped, cut, and ligated. (From Word, 2012, with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


