24
Skin
Chapter map
Skin disorders are common in children. The infant’s skin with its thin epidermis and immature glands is particularly liable to infection and blistering. Birthmarks, rashes and eczema are common in pre-school children. The incidence of skin disease declines until adolescence when acne is common. Skin manifestations are seen in a number of systemic problems, which are covered elsewhere in this book, and pointers to the appropriate chapters are included.
24.2.2 Cradle cap (seborrhoea)
24.2.7 Urticaria (hives, nettle rash)
24.5 Other skin problems covered elsewhere
24.1 Birthmarks
Birthmarks involve blood vessels (naevus, haemangioma) or an excess of pigment in the skin. Haemangiomas are malformations of blood vessels, not neoplasms.
24.1.1 Naevi
The main types of naevi are described below.
24.1.1.1 Stork marks
So named because their position fits with the idea that babies are brought by storks (now discredited!), these are flat, pinkish capillary haemangiomas between the eyebrows, on the forehead and eyelids and on the nape of the neck. They fade gradually over the first 2 years (Figure 24.1).
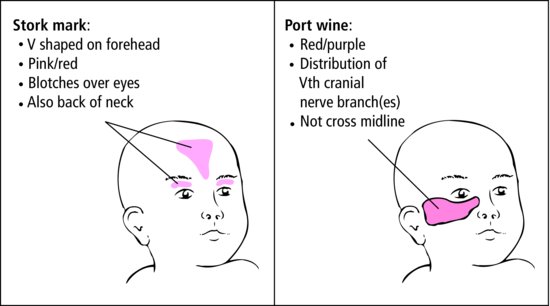
24.1.1.2 Port wine stain (naevus flammeus)
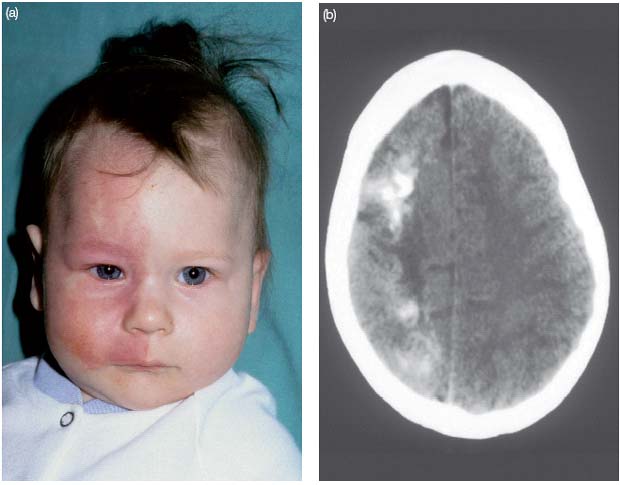
Port wine stain is a capillary haemangioma (Figure 24.1). In the infant, it is flat and pale pink and easily overlooked, but it then darkens to form a flat purple patch of skin which is unsightly. It does not fade. Treatment is difficult. Good results have been achieved using laser, but camouflage with cosmetics is often the best treatment. Sturge–Weber syndrome is a rare association of a unilateral port wine stain of the face (usually in the area of the first division of the trigeminal nerve) and an intracranial haemangioma of the pia-arachnoid on the same side (Figure 24.2). Affected children may present with seizures, hemiplegia, learning problems or glaucoma.
Figure 24.2 Sturge–Weber syndrome: (a) the naevus flammeus and (b) CT abnormality (the white areas in the cortex).
24.1.1.3 Strawberry mark
This is a soft, raised, bright red capillary haemangioma (Figure 24.3). Sometimes it involves deeper tissues and is combined with a cavernous haemangioma which gives it a blue tinge. Common sites are the head, neck and trunk. It appears in the days after birth, and enlarges in the first 6 months to form a raised red lesion. White areas develop in the lump (so that it looks like a strawberry) and it gradually becomes paler and flatter. They nearly all disappear completely before school age. Parents need reassurance. Some that block vision, interfere with feeding or are extremely unsightly may be treated medically or surgically. Spontaneous regression does not leave a noticeable scar, whilst treatment often does.

24.1.2 Abnormal pigmentation
Moles usually develop after the age of 2. They are common and rarely cause anxiety. Single café-au-lait spots are without significance, but six or more patches greater than 0.5 cm in diameter suggest neurofibromatosis (Section 17.4). Pigmented and de-pigmented lesions are seen in tuberous sclerosis (Section 17.4).
24.1.2.1 Albinism
Albinism is a group of genetically determined metabolic disorders with deficient pigmentation. In white people, autosomal recessive varieties affect the skin, hair and often the eyes. In black people, autosomal dominant, partial albinism is more common and does not affect the eyes.
24.1.2.2 Mongolian blue spots
These are large blue-grey patches, most common over the lumbosacral area and buttocks. They are very common in infants of oriental, Asian or black ethnic groups, but rare in white children. They gradually fade and are rarely visible by the age of 10.
 PRACTICE POINT
PRACTICE POINT24.2 Rashes
24.2.1 Napkin rash
This is common in infants. An erythematous rash affects the convexities of the buttocks, inner thighs and genitalia. The skin creases, which do not come into contact with the nappy, are spared. At its simplest, it may merely be an irritant rash caused by wet nappies. Fresh urine does not injure the skin, but prolonged contact with stale urine which has broken down to form ammonia products does (ammoniacal dermatitis). In severe cases, papules and vesicles form which ulcerate, leaving a moist surface which easily becomes secondarily infected with either pyogenic organisms or Candida.
Infection with Candida usually involves the skin creases. It causes an erythematous rash with oval macules, a pimply margin and scattered satellite papules (Figure 24.4).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


