7 Settings of Care
In thinking about where your child will die, at home or in the hospital, you have to contemplate something that is utterly heartbreaking. Recognize that you are doing the hardest, most selfless, and most loving work a parent ever could do. Take credit for that.1
—Joanne Hilden and Daniel Tobben
This chapter explores the settings in which children with life-threatening conditions and their families receive palliative care. It is not uncommon that at different points in the illness trajectory, patients may be treated at different sites such as hospitals, home care facilities and agencies, chronic care facilities, with different teams of clinicians in each setting. Care also extends to respite, schools and other community venues where the children continue to live their lives. The medical home, as described by the American Academy of Pediatrics2 has particular relevance for these children. It is a model of delivering primary care that is accessible, continuous, comprehensive, family-centered, coordinated, compassionate, and culturally effective. The aim of the medical home is to support the needs of children in the home through collaboration among families, clinicians, and community providers. There are statewide initiatives for developing and implementing the medical home model throughout the country.
Epidemiological Factors in Death in Childhood
Despite significant advances in medicine, and the ensuing reduction in mortality rates in children over the past 25 years, children still die (Figs. 7-1 and 7-2). This is attributed to a number of improvements and advances in pediatric health care, including:
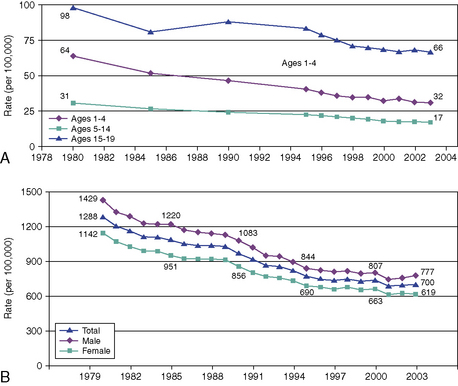
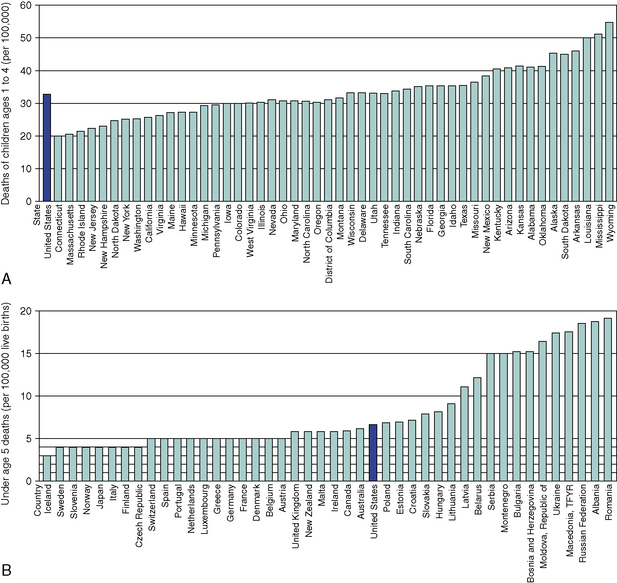
Fig. 7-2 A, Deaths of children, ages 1-4, by state. B, Under age 5 deaths, (by country, per 100,000).
(Data adapted from Field MJ and Behrman RE, eds. “Patterns of Childhood Deaths in America,” Institute of Medicine of the National Academy of Sciences, the National Academy of Press:2003, pp 41-71.)
A 2003 Institute of Medicine report3 estimates that there are approximately 55,000 deaths of children younger than 18 years per year, compared to more than 2 million adult deaths per year in the United States. Approximately, 51 percent of those children die in the first year of life (34 percent in the neonatal period and 17 percent from one month to 12 months of age), 10 percent from 1 year to 4 years of age, 14 percent from 5 years of age to 14 years, and 25 percent from 15 to 19 years of age. In addition there is a large group of young adults (ages 20 to 24), who succumb to chronic debilitating pediatric diseases.
The causes of death vary and are age-dependent: birth defects, low birth weight, maternal complications, respiratory distress, and sepsis account for the majority of deaths in the first year of life. Unintentional injuries, homicide, suicide, cancer, heart disease, and sudden infant death syndrome account for more than 51 percent of pediatric deaths. There still remains a large category of other causes, accounting for 18 percent of pediatric deaths.3
Conditions appropriate for pediatric palliative care fall into one of the following groups:
The Hospital
As children live for longer periods, the need for complex services also escalates.3,6–9 In addition to multiple visits to sub-specialty clinics, many of these children have prolonged and repeated hospital admissions. Whatever the nature and duration of the admission, hospitalization exerts extraordinary psychological demands. The child’s physical distress, and the parents’ witnessing of that distress, is compounded by the implications of the illness that necessitate hospitalization, and by the separation from normal life and from other family members, especially siblings or other children.10 Counterbalancing these stressors, particularly for children with illnesses who have required frequent and prolonged admissions, is the sense that the hospital clinicians become a second family who understand and share in the family’s experiences. Hospitals are a place where many children with life-threatening illnesses and families live, often for prolonged periods.
The Intensive Care Unit
The majority of children (more than 56 percent) die in hospitals and more than 85 percent of these deaths occur in the ICU.3,7 These ICU settings include neonatal (NICU), pediatric (PICU) and more recently created cardiovascular (CVICU) units. Exceptions include tertiary children’s hospitals with end-of-life programs that work collaboratively with community resources.11 A retrospective analysis of deaths in a Canadian tertiary care children’s hospital over a 21/2 year period studied children who were hospitalized for at least 24 hours prior to their deaths and those who were hospitalized for at least 7 days prior to their deaths.12 Acutely ill children who were previously healthy were excluded. Demographic data included age, gender, primary diagnosis, location of death, pain and symptom management, communication at end of life including CODE status, family preference for location of death, and the child’s involvement. Of the 236 deaths, only 86 met study criteria. Neonates accounted for 56 percent of the deaths; in 8, death was unexpected. The ICU saw 83 percent of the deaths and 78 percent of those children were intubated at the time of death. More than half, 57 percent, were medically paralyzed and 3 were on extra-corporeal membrane oxygenation (ECMO). Opioids were administered, mostly by continuous infusion, in 84 percent of the children for pain, dyspnea, discomfort related to mechanical ventilation, or post-operative pain. Acetaminophen, non-steroidal anti-inflammatory drugs and complementary medications were also used, as well as non-pharmacologic therapy, including relaxation and imagery.
A retrospective analysis reviewed the hospital care required for 9000 children and young adults with complex chronic conditions (CCCs) during their last year.8 Children with these conditions accounted for one-fourth of all pediatric deaths. More than 84 percent were hospitalized at death and 50 percent received mechanical ventilation during their terminal admission. Neonates who were less than 7 days of age spent 92 percent of their lives in the hospital; those aged 7 to 28 days spent 85 percent; and infants between one month and 1 year of age spent 41 percent of their lives in the hospital. In the non-neonates, 55 percent were hospitalized at death, with 19 percent mechanically ventilated. The rate of hospital use increased overall as death approached.
This study8 also found variability as to whether children’s code and resuscitation status had been addressed. Discussion about code status was documented only for 79 percent of patients. Results demonstrated that multiple discussions with families were required regarding resuscitation and an actual Do Not Resuscitate (DNR) order. Once a DNR decision was obtained, the majority of children died within one day, although some children lived as long as 30 days. In charts without documentation of DNR status, cardiopulmonary resuscitation was initiated but was unsuccessful.
The mode of death in a number of PICUs has been well described.13–18 A decision to forgo life-sustaining treatments was made in only 20 to 55 percent of critically ill children who eventually died. Diverse cultural, religious, philosophical, legal, and professional attitudes often affect these decisions. Despite the children’s grave prognoses, CPR was initiated and had a failure rate that varied from 16 percent to as high as 73 percent. Full life support at the time of death varied from 18 to 55 percent of the patients. A DNR order was found in less than 25 percent of the patient’s charts. Withdrawal or limitation of life-sustaining therapy, including extubation, occurred in 43 percent of the patients. More than 90 percent of these children died within 24 hours; the rest died on the second day.
The Intensivist’s Role
The intensivist must engage the family in ongoing discussions about end-of-life issues and repeatedly address and evaluate the goals of care.5 This role continues long after decisions to forgo life-sustaining treatments have occurred, as families look to the attending intensivist throughout the dying process. The ICU team assures the family that the child’s care is undertaken with a focus on quality of life, dignity, and comfort.19,20 The ICU nurses play a central role; at the bedside, families often call upon them for explanations of the child’s care and the existing options as well for emotional sharing.21 This is also where the social workers, psychologists, child life specialists, and chaplains of the interdisciplinary team can play pivotal roles. Studies have shown that when the ICU staff spends time conversing and providing bereavement resources, the families experience less stress, anxiety, and depression after the child’s death.22
Decision-Making in the ICU Setting
The decision-making process is often extremely difficult and may require many meetings and interdisciplinary care conferences with the family. The process may be divided into three steps: deliberation, eventually leading to the decision and goal setting; implementation; and evaluation of the decision and its application.23–25 During the deliberation, the family’s decision makers and the clinical teams must weigh the benefits and burdens of various options in terms of survival, long-term outcomes, and quality of life for the child. The concept of shared decision making allows for a consensus to be reached by all active participants once the pertinent information has been shared. It should enable the family to make a truly informed consent.
Cardio-pulmonary resuscitation
The use of cardio-pulmonary resuscitation (CPR) has had enormous impact on children’s care. Unfortunately, providing CPR for both acutely and terminally ill patients is not as beneficial as had been hoped, because less than 27 percent of children who arrest in the hospital survive to discharge. Some advocate CPR should be reserved only for those children with truly reversible medical conditions.26 Nonetheless, with the use of more invasive procedures in critical care, more children may be resuscitated onto an ECMO circuit following a cardio-pulmonary arrest. This intervention may indeed improve survival, but is associated with the high risk of neurologic injury.27,28 Clinicians should inform families about the risks and benefits of CPR. It is also crucial that the family be reassured that a Do Not Resuscitate order does not mean the cessation of care for the child. Rather, it indicates a shift in priorities, toward the implementation of more comfort interventions for the child.29–31
Withholding or withdrawing life-sustaining support
The decision to withhold or withdraw life-sustaining treatment is always difficult. While they are considered to be ethically equivalent, physicians seem to be more comfortable with withholding; withdrawing may increase a sense of responsibility for a patient’s death. The minimizing and eventual withdrawal of technology increases opportunities for the family to hold the child. Parents may hold and cuddle their child, or lie in bed and comfort the child during this transitional period. The process of withdrawal of technological intervention requires a team effort and an environment that is supportive for the family. A room that provides privacy for the family, while also shielding other patients and families in the intensive care unit, is beneficial.5,13,32,33
Compassionate extubation
Families’ questions about what to expect when a terminal, or compassionate, extubation is planned revolve around whether the child will feel pain or suffer, be conscious, or breathe. Liberal use of sedatives, analgesics, and anxiolytics should prevent most negative symptoms. Families must be prepared for different scenarios that could unfold; however, no sure predictions can nor should be made regarding when their child will die. Certain children will die shortly after extubation, including those who are brain dead, in severe refractory shock, or in severe respiratory failure with refractory hypercarbia and hypoxia. Children who are not brain dead may linger for hours, days or longer, with variable respiratory patterns. If the parents or nurses perceive the child to be uncomfortable, then opioids and/or benzodiazepines should be given; for children who are difficult to sedate, propofol or pentobarbital may be used. Pain and suffering should be treated aggressively, even if this results in a foreseen unintended hastening of death. This principle is referred to as the “doctrine of double effect.”33–35
Withholding or withdrawing medically provided nutrition and hydration
Although not a frequent issue in the ICU, pediatricians often have a difficult time with this aspect of terminal care and benefit from team discussion. Arguments that have been made for continued hydration and nutritional support are that children have a remarkable ability to recover, infants need assistance with feedings, and very little is known about whether or not a child at the end of life willfully refuses food and water. The American Academy of Pediatrics concluded in 2009 that the withdrawal of medically administered fluids and nutrition for pediatric patients is ethically acceptable in certain circumstances.19
Autopsy
Although it is often difficult to request an autopsy, it may provide the parents and clinicians with more information about the child’s illness and death. An autopsy may be all-inclusive or limited to those organs most involved in the disease process. Many clinicians have found the request for autopsy to be more successful if the subject is broached during end-of-life discussions with the family before the child has died. Parents may be too distraught to consent if they are approached for the first time in the immediate aftermath of the child’s death. When an autopsy is performed, it is imperative that one of the physicians who cared for the child review the results with the parents when they feel emotionally ready.36 In addition to providing information, this meeting provides a valuable opportunity for follow-up with the family. If the death is a coroner’s case, then the coroner will make the determination about the post-mortem exam and the potential for organ and tissue donation.
Organ and tissue donation
Most ICUs work closely with an Organ Procurement Organization (OPO), whose professionals are trained to counsel families. In the past, brain death criteria had to be met in order to be a donor. Now, all hospitals must have a Donation after Cardiac Death (DCD) policy. This allows organs to be donated after life-sustaining interventions are discontinued, even when criteria for brain death have not been met. In these instances, it is anticipated that the patient will have a cardiac death within 2 hours in the operating room, and then have the appropriate organs retrieved for transplantation. Although the procedure is designed to increase the number of organs available, it is a cumbersome process and involves many additional steps and significant waiting times. If the patient does not sustain a cardiac death in the requisite time for donation, the child must be returned to the ICU or another in-patient area for ongoing care.32–34
Emergency Medical Services
Unintentional injury remains the leading cause of mortality among children age 1 to 19 years, accounting for 44 percent of deaths.40,41 Thus, from an epidemiologic perspective, the dominant trajectory of childhood death is sudden and unexpected.42 An estimated 20 percent of childhood deaths actually occur in the emergency medical services (EMS) environment.43,44 Myriad pediatric palliative care issues face clinicians in the EMS, a setting where all trajectories of pediatric life-threatening conditions may intersect. As a result of biomedical, procedural and technologic advances, many children with complications of prematurity, congenital malformations, complex chronic, and life-threatening diseases are surviving longer and living in community-based settings such as sub-acute care facilities or at home. Physiologic exacerbation of an underlying disease state, intermittent infection risk and/or mechanical complications of technology dependence all require immediate attention, and present a spectrum of palliative care challenges to staff. This section will focus on sudden and unexpected death in childhood, and elucidate:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


