18 Self-Care
The Foundation of Care Giving
The best way to become a better “helper” is to become a better person. But one necessary aspect of becoming a better person is via helping other people. So one must and can do both simultaneously.1
As clinicians come face to face with the inevitable suffering of a child’s dying and death, they have a choice, if not always consciously made, in how they approach their work. When they cope with suffering by seeing themselves as strong and giving to others who are perceived as weak, they are at high risk for burnout, becoming disillusioned and drained of energy. By contrast, if instead of helping the weak and vulnerable, they choose to offer themselves in service, then they assume a role of knowledgeable guide. As a knowledgeable guide they serve others with their whole selves that includes their particular strengths as well as vulnerabilities. Clinicians recognize the dark, the light, and the weak and strong aspects of their being and understand that are all needed in situations of intense suffering. They also recognize that despite their specialized knowledge in some areas, in most areas they share the sense of mystery experienced by those they serve. They can do only what they can, then they must let go of expectations that they can control outcomes that never were within our control. If they perceive their work as offering their whole selves in service, then the necessity to work on themselves becomes apparent. This self-work or self-care is both a requirement of their roles as well as a privilege they are being offered: to be allowed to become more themselves and to move toward their own potential as part of their daily jobs. As Robert Coles said, “I had begun to see how complicated this notion of service is, how it is a function of not only what we do but who we are (which of course, gives shape to what we do).”2
What do care givers have to offer families of children who live with a life-threatening illness? What more can they possibly do or say when all has been done in terms of pain and symptom control? How can each of the care givers be enough in the face of such suffering? They know that what children and parents value during these times is the abiding presence of a trusted person who listens and bears witness to their suffering, even better if that person has experience in being present in similar life-threatening situations, and has walked that path with others.3,4 “All I want is what is in your mind and in your heart,” said dying patient David Tasma to Cicely Saunders, founder of the modern hospice movement. Tasma shared and supported her dream to develop a hospice. The quality of care is not limited to professional expertise but is greatly affected by what each clinician, as individuals and as members of a professional team, brings into relationships with children, adolescents, and parents. While bringing their imperfect selves to the service of others is necessary, it is not, however, sufficient. What is also required is that clinicians care for themselves in an ongoing reflective and systematic way.
The term self-care has been used in a variety of activities and in its most reductive sense is understood superficially as taking time for ourselves or taking a vacation. While it is important to balance work-life with other activities, the kind of self-care that leads to enduring personal resilience and growth requires more than time away because clinicians can never get away from themselves. In the words of Jon Kabat Zinn, “Wherever you go, there you are.”5 Self-care, when stripped of self-reflection, meaning making and paying attention in the present moment, becomes a self-centered exercise that is about I, Me, and Mine. Self-care activities based solely on distractions, such as vacations and other means to get away from work, can become selfish. If distractions and running away, including reliance on drugs and alcohol, are exclusively what self-care consists of, then inevitably there is never going to be enough time away. When the habit of running away from what is in the present moment becomes an established practice, then caregivers find that each distraction is good for a while but inevitably tolerance develops and no time away or distraction is ever enough. It is important to clarify that distraction, in and of itself, is not bad or unhealthy; and when entered into mindfully it is one of many strategies that can be helpful. Rather than being harmful, distraction, in the correct balance, is necessary but not enough to encompass the self-care needed in pediatric palliative care. While eating well, getting adequate sleep, regular medical care, physical exercise, having interests outside work, and making time for oneself are all important and necessary aspects of self-care, they are not sufficient. What follows in this chapter is a focus on the deep work of caring for the caregivers, which is essential when attending to the suffering of others.
Relationship to Self
All of that is possible in the context of relationships that are personal. Personal relationships both make the job highly stressful but also deeply fulfilling, and determine the degree of satisfaction that families experience with regard to the care being offered to them. We have come to understand that the relationships developed with the parents of seriously ill children are often problematic, and professionals who are insensitive, unavailable, or impersonal in their approaches elicit parental dissatisfaction and increased distress.3,6–13 Parental satisfaction with care is directly related to the nature of the relationships held with the care providers. These relationships have a positive or negative impact upon how families experience the dying process and death of a child, and seem to affect their long-term adjustment to loss. These findings make self-reflective practice a necessary part of the job, and encourage caregivers to review the relationships developed as well as challenge some of the mistaken beliefs according to which specialized knowledge, refined skills, and clinical experience are thought to be enough to ensure quality of care. While knowledge, skills, and experience are undoubtedly critical, families of seriously ill children demand more than that and expect a personal, human, and caring relationship. The following example illustrates how quality of care extends beyond the provision of expert care, and encompasses the development of nurturing and meaningful relationships with children and parents.
A Relationship-Centered Approach to Care
Papadatou14 suggests that it is necessary to expand our view of the care of seriously ill children beyond the family-centered approach that limits focus to the needs, concerns, and preferences of young patients and their families. This broader outlook is possible if a relationship-centered approach is adopted. Such an approach illuminates the dynamics that develop in life-and-death situations among patients, family members, professionals, and teams, and considers the larger organizational and sociocultural contexts in which care is offered and received. It explores the reciprocal influence of patients, families, and professionals and sheds light upon their subjective experiences and interactions in the context of healthcare.15 In essence, the relationship-centered approach focuses on whatever transpires when the private and social worlds of a sick child or family interacts with the private and social worlds of care providers in a given work and social environment. To better understand the outcomes of such encounters, it is important to consider its basic components (Fig. 18-1):
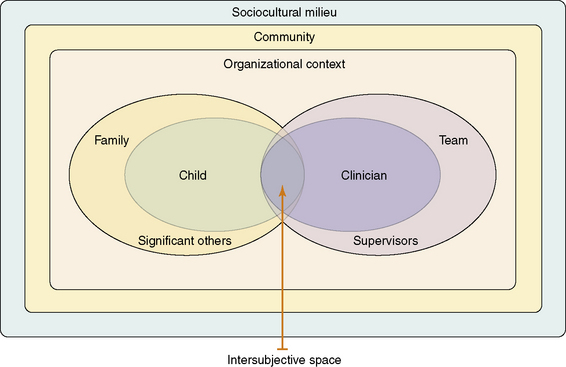
According to Stern,16 the intersubjective space is “the domain of feelings, thoughts, and knowledge that two (or more) people share about the nature of their current relationship” (p. 243). When the clinician and the patient or parent are open to each other, and to their respective worlds, then the intersubjective space is enlarged to include a rich partnership, a fruitful collaboration, and the co-creation of new narratives. It also includes opportunities for increased self-awareness, new learning, positive changes, and personal growth in the midst of uncertainty and hope. Such experiences render the process of care human, meaningful, and rewarding. By contrast, when both clinicians and family members enact prescribed roles and focus solely on what needs to be done, which is often accomplished in a ritualistic or detached manner—then the intersubjective space becomes limited in its capacity to offer opportunities for genuine connection. It is also limited for viewing reality in a new way, and for containing, tempering, and transforming suffering in meaningful ways while developing resilience in the midst of adversity and loss.
The Private Worlds of Professionals
These beliefs prevent clinicians from developing caring relationships in which they are fully present and aware of what unfolds in the intersubjective space that is shared between themselves and others. As caregivers, knowing oneself is equally important as knowing the child, the adolescent, or the family to whom services are provided. Such ‘self-knowledge’ should not be limited to cognitive understanding, but also includes the integration of information gathered from emotional responses, physical senses, and bodily reactions, all of which contribute to self-understanding. When caregivers accompany families through illness, dying, and bereavement they cannot promise a cure, a perfect death, or recovery from bereavement. All they can assure is a committed and authentic relationship in which they will strive to remain fully present and open to the child’s and family’s experiences, no matter how painful or distressing these may be. According to Papadatou14 such openness “permits us to meet the unknown in life, in others, or in ourselves without preconceived ideas or rigid theories and planned interventions. It allows us to welcome the unexpected without always trying to provide a logical explanation, and to work through the paradoxes that are inherent in life and death situations.… This process demands time, energy, and commitment. When we are consumed by the everyday and rush from one activity, task, or crisis to the next, we do not engage in a deep examination of our experiences and we restrict our capacity to provide effective care and to reap the rewards.”
When caregivers remain open and vulnerable enough, they acknowledge the presence of death in all relationships and cope with its effects upon patients, families, teams, and themselves. Only then may they recognize its violent impact upon relationships which are threatened, broken, or severed forever, as well as its vitalizing force that motivates families to live more fully and confronts us with life’s value and meaning.14,17
What are some aspects of caregivers suffering?
Suffering That Leads to Impairment
Burnout is a “state of physical, emotional, and mental exhaustion caused by long-term involvement in emotionally demanding situations.”18 Although described as a static state, burnout is more of a process that develops gradually, when:
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


