Chapter 38 SCROTAL MASSES
General Discussion
The most common painless scrotal masses in infants, children, and adolescents include indirect inguinal hernias, hydroceles, varicoceles, and spermatoceles. Testicular tumors, perinatal testicular torsion, acute idiopathic scrotal edema, and soft tissue tumors of the spermatic cord are less common causes. Figure 38-1 provides a clinical approach to the painless scrotal mass.
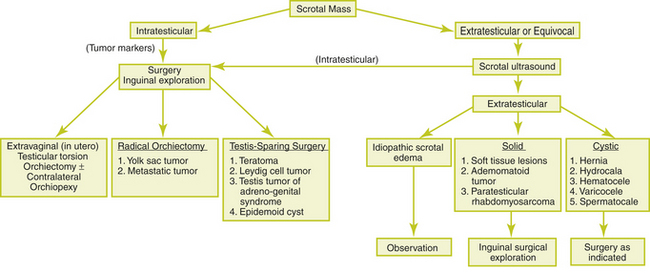
Figure 38-1 Clinical approach to the painless scrotal mass.
(From Skoog SJ. Benign and malignant pediatric scrotal masses. Pediatr Clin North Am 1997;44:1229-1250, with permission.)



