CHAPTER 35 Sacrococcygeal Teratoma
Step 1: Background and Surgical Anatomy
♦ Sacrococcygeal teratomas (SCTs) are the most common extragonadal germ cell tumors in children. The incidence is approximately 1 in 35,000 live births, with females accounting for 75% of cases.1
♦ SCTs are composed of elements from one or more of the embryonic germ cell layers and contain tissue foreign to the anatomic site of origin. Mature teratomas consist of well-differentiated tissues, whereas immature teratomas contain varying amounts of immature tissue such as neuroectoderm.2 Histologically, teratomas are classified according to their stage of immaturity.3


♦ When the tumor is found before 1 month of age, the risk of malignancy is about 5%, whereas when the tumor is discovered between 1 and 12 months of age, the risk of malignancy is 60%; in children older than 1 year, 75% of tumors are malignant.3
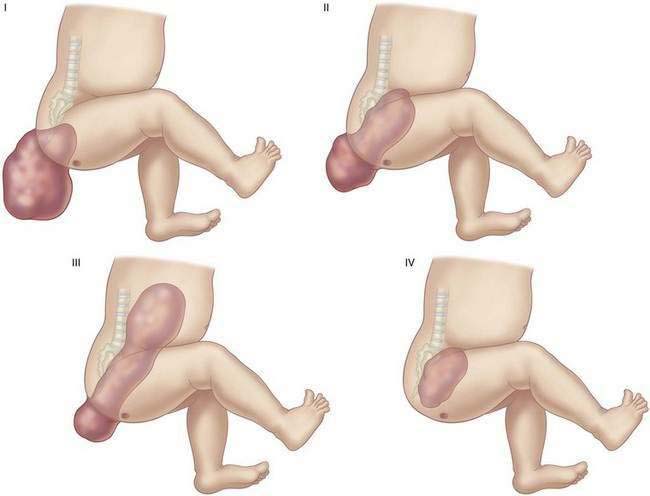
♦ The most commonly applied anatomic classification, adopted by the American Academy of Pediatrics (AAP), is based on the degree of intrapelvic extension (Fig. 35-1).4
Step 2: Preoperative Considerations
Neonatal
♦ Generally the tumors are noted to have a characteristic mass protruding from the sacral region (Fig. 35-2).
♦ This lesion is often detected by prenatal ultrasound. If the external portion is larger than 5 cm, abdominal delivery should be considered so as to avoid dystocia and tumor rupture.2

Infant and Pediatric Patients
♦ Generally older children have no external portion noted at birth and present secondary to tumor compression of the bladder or rectum or a palpable rectal mass.
♦ Preoperative evaluation should focus on evaluating the degree of pelvis and abdominal extension by the following:
 Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region
Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region
 Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3
Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3
 Laboratory investigations: An elevated serum alpha-fetoprotein (AFP) level is commonly associated with malignant tumors (yolk sac or endodermal sinus tumor, embryonal carcinoma, or undifferentiated germ cell tumor).2
Laboratory investigations: An elevated serum alpha-fetoprotein (AFP) level is commonly associated with malignant tumors (yolk sac or endodermal sinus tumor, embryonal carcinoma, or undifferentiated germ cell tumor).2
Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3 Laboratory investigations: An elevated serum alpha-fetoprotein (AFP) level is commonly associated with malignant tumors (yolk sac or endodermal sinus tumor, embryonal carcinoma, or undifferentiated germ cell tumor).2
Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3 Laboratory investigations: An elevated serum alpha-fetoprotein (AFP) level is commonly associated with malignant tumors (yolk sac or endodermal sinus tumor, embryonal carcinoma, or undifferentiated germ cell tumor).2

Table 35-1 Frequency of Malignancy Associated with Higher American Academy of Pediatrics Anatomic Classification
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


