18 Respiratory Problems Asthma is a serious condition that can be life threatening. Most children with asthma we treat are on daily medication to prevent asthma attacks, and often additional medication to help calm down or stop attacks once they begin. Those with milder asthma conditions may be taking the asthma medication only with signs of impending symptoms. Some patients will present with asthmalike symptoms (wheezing, difficulty breathing, chronic cough) due to other conditions such as croup or bronchitis. If these conditions are chronic, the child may have been prescribed asthma medications to help with the difficult breathing or chronic cough. Sometimes parents turn up with their child stating that their child has asthma for which they receive asthma medications, but it is actually a more severe form of something like croup with some of the same symptoms of asthma (wheezing, difficulty breathing). Occasionally, you may find some confusion around the actual diagnosis of the condition that the child has. In this subsection I describe the treatment of asthma and discuss some additional problems that can manifest with asthma symptoms such as croup.1 __________________ 1 A number of similarly manifesting conditions are covered in various chapters in this book. Here I discuss “asthma” with indications for treatment of asthmalike manifestations of something like “croup.” On pages 113f I discuss a number of other respiratory conditions, which can also include similar manifestations of signs and symptoms. In chapters 25 and 26 I also discuss treatment of underlying conditions that can predispose towards these problems. Case 1 Main complaints: He had been coughing daily for a long time. The condition had been diagnosed as asthma for which he had been prescribed the daily use of a steroid inhaler. He had a tendency to catch cold easily, the cold triggering worsening of the asthma symptoms, especially the coughing. His sleep was poor as he was woken many nights by the coughing. History: He was born 6 weeks premature and was in hospital for the first 10 days of life. It was felt that his condition was probably a result of being born premature. Diagnosis: From the symptoms and the pulse (right pulse weaker than left), I diagnosed him as having the lung vacuity pattern. Treatment: I discussed with the mother how to test for cow’s milk sensitivity (see Chapter 17) and she agreed to start this as soon as possible. Tapping with the herabari was applied on the head, GV-12 area, neck area, and a little on the back. Stroking with an enshin was applied down the arms, legs, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-5, draining to right LR-3 and left TB-5. Still using the teishin, light stroking was also applied down the back. Press-spheres were left on left BL-13 and the “stop coughing” points on the elbows. Second visit—7 days later No coughing at all this week. The coughing had stopped immediately after treatment. As a result of the dramatic change, his mother had stopped giving him the inhaler, so that he had not used it at all this week. However, his sleep was not so good and he had woken in a bad mood several mornings. Treatment: I spoke to the mother about the wisdom of simply stopping the use of the inhaler and that she should at least consult with the prescribing doctor. She agreed to consider this. Tapping with the herabari was applied to GV-20, the neck, GV-12, LU-1, and occipital regions. Stroking with an enshin was applied down the arms, legs, and abdomen. Using a teishin supplementation was applied to left LU-9 and SP-5, draining to right LR-5 and TB-5. Press-spheres were left on right BL-13 and the “stop coughing” points on the elbows. Third visit—5 days later He woke on this day with a cold at 5.30 a.m. with symptoms of coughing. He was still coughing, but with signs of improvement. He had diarrhea over the weekend as well. Treatment: Tapping with a herabari was applied to GV-20, ST-12 region, neck region, LU-1, GV-12, and LI-4. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-3, draining to right LR-3. Press-spheres were left bilaterally on the asthma shu points and GV-12. Fourth visit—2 weeks later His cough was much better, but he was still coughing a little in the early morning. Treatment: Tapping with the herabari was applied to GV-20, ST-12 region, GV-12, and LI-4. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to right LU-9 and SP-3, draining to left LR-3. Press-spheres were left on bilateral asthma shu points and behind shen men on the back of the left ear. Fifth visit—1 week later The cough was much better again, but he had started coughing a little more 2 days before this visit. Treatment: Tapping with the herabari was applied to the head, ST-12 region, occipital region, LU-1. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-3, draining to right LR-3. Press-spheres were left bilaterally on the asthma shu points and behind shen men on the back of the left ear. Sixth visit—13 days later The cough had again improved, but he had started coughing a little more in the early morning with a cold that started 1 day before this visit. Treatment: Tapping with the herabari was applied to GV-20, ST-12 region, LU-1, GV-12, LI-4, and LI-11. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-3, draining to right LR-3. Press-spheres were left bilateral on BL-13 and behind shen men on the back of the left ear. Seventh visit—2 weeks later No symptoms of coughing and his condition was overall much improved. There were no sleep disturbances. Treatment: Tapping with the herabari was applied to GV-20, ST-12 region, GV-12, LI-4, and LI-11. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-3, draining to right LR-3 and left SI-7. Press-spheres were left on GV-12 and behind shen men on the back of the left ear. Eighth visit—22 days later On holiday he started with a lung infection and was prescribed antibiotics. He fully recovered and had had no coughing before or since then. This was a significant milestone, since any time he had got sick like this before his cough had severely worsened. This time, he had no coughing! Treatment: Tapping with the herabari was applied to GV-20, the neck region, GV-12, and LI-4. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to left LU-9 and SP-3, draining to right LR-3. Press-spheres were left on GV-12 and behind shen men on the back of the left ear. Treatment finished as the family moved away. In the final discussions with his mother she revealed that she had not talked to the doctor who had prescribed the inhaler. She had always kept it with her, but since the first visit Gilbert never needed the inhaler. She was very happy with treatment and promised to contact me for a referral should the need arise in the future. Reflection: In a case like this, one cannot determine the degree to which improvement is possible. It is possible his lungs were weakened due to having been born premature. It was also possible that he was sensitive to cow’s milk products, and that eliminating them after the first visit had contributed to his improvements. It is also possible that he actually had an asthmalike condition such as “croup” rather than asthma per se. Also, I did not prescribe the mother to do daily home treatment since he was responding so well to treatments. I prefer to use this additional therapy when the condition of the child is not changing or the changes are slow coming. In Gilbert’s case, this was not necessary. Although he caught a few colds during the time he was receiving treatment, none progressed to a major worsening of his symptoms, which I took to be a good sign of the change of his condition. Also, I felt that as well as having a trend toward weak lung constitution he also had a strong tendency toward liver repletion. Hence, even after his sleep problems had improved I continued treating points that would be helpful for this tendency such as the point behind shen men on the back of the ear, GV-12, and so on. Generally when we treat patients who have asthma, we are using treatment to augment or complement the existing therapy that they usually receive—the daily inhaled medications. Asthma is a serious condition that can kill the patient. Since we have no evidence that acupuncture can save the life of an asthmatic patient who is having an asthma attack, we do not use acupuncture in place of the usual drug therapy. While these drug therapies do not generally cure the illness, they help reduce the asthma attacks. Although in the past acupuncturists have had to try using acupuncture to stop asthma attacks when such medications did not exist, we do not usually do this. The principle goal of acupuncture treatment of an asthmatic child is to slowly change the overall condition of the child so that he or she is less prone to having asthma attacks in the future. In other words, most of our work is preventative. This does not mean that we cannot use specific techniques or acupoints to try to keep the asthma symptoms quieter, reducing the frequency or severity of attacks, but our primary goal is to use the root treatments, both pattern-based and core non-pattern-based, to change the overall condition of the patient. Thus, if the patient has an asthma attack in your clinic, it is advisable to wait for the parent to administer the inhalant medication to the child. Once the attack has calmed down you can start to apply your treatment on the child. In a baby or young child, where full diagnostic examination can be more difficult, it is advisable to focus on the symptom as the constitutional type of the patient and thus treat the lung vacuity pattern. If the child is a little older and has a longer history of taking medications for the condition, it is possible that the pattern has changed. If you are able to get more detailed information from the pulses and other methods, you can follow the pattern that emerges. In my experience kidney or liver vacuity patterns seem to emerge. One of my teachers, Akihiro Takai suggested that with extended use of steroid medications the patient can start to show the kidney vacuity pattern. Check for softer or cooler lower abdomen and cool feet, as well as the specific pulse findings. Sometimes the liver seems to become reactive to the extensive use of medications and the liver vacuity pattern emerges. To check for this as well as the usual liver pulse findings, check to see if the right subcostal area has started to become stiffer than the left or is more sensitive or jumpy than the left. For the lung vacuity pattern we usually treat LU-9 and SP-3, but following the ideas of Nan Jing (Classic of Difficulties) Chapter 68, it can be helpful to try the jing-river/metal points LU-8 and SP-5 instead if the child presents with cough. The usual treatment of the kidney vacuity pattern already uses the jing- river/metal points KI-7 and LU-8. But if the feet are very cold and the child appears flushed, try the he-sea points KI-10 and LU-5 (following Nan Jing Chapter 68 again, which indicates he-sea points for counterflow qi). Because the primary goal of treatment for an asthmatic child is to try to change the underlying condition, it will be important to apply some form of pattern-based root treatment along with the core non-pattern-based root treatment. The two complement each other very well, and with minimal symptomatic treatment, one can see rapid changes in the asthma symptoms in most children. Apply either the whole body tapping treatment or the combined light stroking with targeted tapping treatment as the core non-pattern-based root treatment (Fig. 18.1). As soon as it is feasible, it is very helpful to have the parent start applying a simplified form of this on the child regularly at home. Usually, you can start the home treatment by the second or third treatment session. However, some children have concurrent skin problems in addition to the asthma symptoms. This makes it more difficult to decide how to apply some simple treatment at home. If the child has very congested lungs, usually with rapid breathing and cough that is worse at night, focus the light stroking and tapping to the chest region, until it starts becoming slightly redder, then to other body areas. In addition to the core non-pattern-based treatment you can add additional tapping to specific areas such as around LU-1, on the chest around CV-17, the interscapular region around GV-12, LI-4, the shoulders, and the supraclavicular fossa region. Shimizu (1975) also recommends applying light treatment to acupoints such as LU-5, LU-6, KI-6, KI-7 when the lungs are very congested. For older children with asthma or asthmalike symptoms contact needling (light tapping or rubbing) can be applied to acupoints such as KI-16, LU-1, CV-16, CV-14, LR-14, KI-26, BL-11, BL-13, BL-17, BL-23, GV-12, GV-10, LU-5, KI-6 or KI-7. Palpate and select reactive points for treatment. If you have applied a pattern-based root treatment to the lung or kidney channels, it may be advisable not to additionally apply these symptomatic treatments to the lung or kidney channel points on the limbs. Fig. 18.1 Usual stroking plus tapping: • Supraclavicular fossa region: five to 10 times • Around LU-1, CV-17: 10 times each • Around LI-4: five to 10 times each side • Around GV-12: 10 to 20 times If the child is over-sensitive, Shimizu recommends treating acupoints such as GV-20, BL-7 or GB-17, BL-10 or GB-20, GV-12, CV-17; if there is tension in the subcostal and/or substernal regions one can treat CV-14, CV-12, ST-19, ST-21, ST-27, GB-24, LR-14, above LR-14, BL-18, BL-20, ST-36, GB-40. Palpate and choose reactive points for stimulation. If the child has a more weakened body type, the skin of the abdomen is thin, the rectus abdominus muscles stiff, there are fluid sounds in the stomach on percussion of the abdomen, treat KI-21, KI-19, lateral to CV-9, KI-16, KI-15, SP-16, BL-20, BL-23, BL-51, KI-7 (palpate and choose reactive points for treatment) (Shimizu 1975). The asthma shu point is an extra point. It is located slightly lateral to BL-17 and slightly superior to the level of BL-17 (see Chapter 16, p. 88). A distinct knot is found on one or both sides in virtually every asthmatic patient palpated. You will find it useful on almost every asthmatic patient to keep this point stimulated. For treatment either place press-spheres, the new press-tack needles, or intra-dermal needles. As described in Chapter 12, we can use these different tools interchangeably. The press-sphere generally applies a lower dose, the new press-tack needles (0.3 mm and 0.6 mm) apply a slightly larger dose, and the intra-dermal needles a larger dose again. Thus, on the first visit or for the more sensitive child we start by using press-spheres on the asthma shu points. We can increase dosage by starting to use the press-tack needles and increase again by using the 3-mm-long intradermal needles. The dose is also modified by varying the length of time that the treatment tool you have chosen to use is retained. Often the press-tack needles or intra-dermal needles are removed that night, by the next morning, before bed the next day, or on the morning after that. Since it is good to keep the asthma shu points stimulated in order to help keep the asthma symptoms quieter, once the press-tack needles or intra-dermal needles are removed, you can have the parent replace them with regularly changed press-spheres. To judge which tools to use on a particular child, it is necessary to examine the condition of the child and also track the progress of treatment. For example, in a stronger-bodied 2-year-old child who is not excessively sensitive you can use the press-spheres or intra-dermal needles sooner. As described above, the asthma shu point is commonly treated and kept stimulated with press-spheres, press-tack needles, intra-dermal needles, or a combination of these. Additionally, GV-12 is a good point to place a press-sphere. Other points that can be helpful to keep the asthma symptoms quieter (less frequent, less severe attacks, greater ease of breathing between attacks) are points like BL-13, LU-1, KI-25 to KI-27. On the young child who is still in the more oral phase, retaining press-spheres, press-tacks, or intra-dermal needles on the front half of the torso can be difficult as the child might pull them off and try to swallow them. Thus, LU-1 and the kidney channel points tend to be used less frequently. When the child has improved and has few symptoms, and has been reducing medication intake, on follow-up treatments where you are still working on improving the overall condition of the child, it can be helpful to retain press-spheres or press-tacks on back shu points related to the pattern-based Meridian Therapy treatment.2 Thus, treatment with these tools can be directed to BL-13 on one side with BL-20 on the other for the lung vacuity pattern; bilateral BL-23 or BL-23 on one side and BL-13 on the other for the kidney vacuity pattern; and BL-18 on one side, BL-23 on the other for the liver-vacuity-related pattern. __________________ 2 This treatment model is outlined in Birch and Ida (1998, pp. 158–159). If the asthma manifests with coughing, check for the “stop coughing” extra point, which is located just distal and lateral to the TCM LU-5 location. This point, if hard and uncomfortable,3 can be treated with press-spheres, or on older children with press-tack needles. __________________ Yoneyama and Mori were applying shonishin treatment in their practices as a form of primary care, since many parents would bring their child to the clinic instead of or before going to the pediatrician. They were also working in situations before the social health system was as well established as it is today. Thus, they had opportunity to apply treatment on children to stop an asthma attack. I mentioned above that we do not usually recommend this course of treatment, but in an emergency you may find yourself having to help, and so you should know what the recommended treatment approach is. For treatment at the time of an asthma attack: shallowly insert thin needles at BL-11, BL-12, KI-27, LI-18, CV-22. It might be easier to insert intra-dermal needles temporarily at those points. One can also add needling to CV-12, CV-13, or CV-14 in the upper abdomen with good effects (Yoneyama and Mori 1964, pp. 68–69). It is useful to know these points as they can also be used as part of your symptomatic treatment approach for the general condition of asthma rather than to target relief of a specific asthma attack. Hyodo (1986) recommends light needling to the following points for the treatment of asthma: BL-11, BL-12, CV-22, LU-1, LU-5. If not needled, they can also be treated with press-spheres to help address the general asthma condition. Shimizu’s (1975) recommendations for asthmatic symptoms of croup include very light in and out needling of acupoints such as KI-26, LU-1, BL-11, BL-13, BL-17, BL-23, depending on palpable reactions. For asthma he recommends CV-22 as an especially effective acupoint. Irie, following his teacher Fukaya (Irie 1980) recommends the following treatment points with moxa for asthma: asthma shu point and GV-12 (three to five moxa each). As discussed above, I have found it easier to use needling, press-spheres, press-tack or intra-dermal needles to the asthma shu points. Manaka has different recommendations for the use of moxa on children for asthma (Manaka et al. 1995, p. 212). He suggests the following points: CV-14, LU-1, LR-14, GV-12, BL-13. For more severe symptoms on older children, Shimizu (1975) recommends applying moxa to points such as GV-12, GV-10, LU-5, or LU-6 (half a grain of rice size, three to five cones per point). In general you will find that you use moxa as a last resort in the treatment of asthma or if the asthma is a product of the child having the lung weak constitution pattern. In this case the moxa may be directed to GV-12 rather than all the above listed points (see Case 1 in Chapter 25, “Weak Constitution”). If the child has chronically congested lungs so that if they cough you can hear the congestion and especially when they breathe you can hear the congestion, it can be helpful to apply cupping over the interscapular region to help break up the congestion in the lungs. Please pay attention to the dose discussions in Chapter 14 around the use of cupping. Thus, for the infant, apply cupping for a few seconds on each occasion with fewer pressure and less places. For the stronger, older child apply the cupping for a few more seconds in each place with more pressure and to more places. The cupping should never cause pain. It is also good to be aware that once you have applied cupping on a child, he or she will usually come to expect it, since they will find it an interesting and enjoyable experience. You may find that in order to please the child on future visits, you need to apply a little cupping even though it may no longer seem necessary. If this happens, make sure to go back to a very low dose approach. On some children with asthma you will find vascular spiders on the upper back, especially up around the lower cervical, upper thoracic vertebrae. On occasion you may need to stab and bleed these vascular spiders in order to get the stubborn symptoms of asthma to start to improve. This technique is discussed in Chapter 15. Shimizu (1975) mentions that bloodletting in the interscapular region can be very effective to help treat asthma. In general we do not apply this very often, mostly when the condition is not responding and you are looking for a stronger technique to try to trigger change in the symptoms. In children with asthma, it is necessary to discuss what the child consumes, in particular cow’s milk products. You will often find that you need to discuss having the parents test sensitivity to cow’s milk products and then to have their child stay away from them. I have often found that the excess mucus production triggered by cow’s milk product consumption is either causally related to the asthma or associated with an irritation of it. Some children have allergic-type asthma that involves airborne allergens. Parents aware of this will usually be doing their best to keep the house clean, vacuuming and cleaning daily. If, however, this is not sufficient to stop the problems you may need to give further advice. I have had some families with a cat or dog that the child is known to be allergic to. The parents cannot give up the animal. If trying to persuade them of the wisdom of letting the animal go does not work, you may need to recommend additional measures to help. The same measures may be needed if daily cleaning and vacuuming seems not to be enough whether animals are present or not. In this case it is a good idea to recommend that they purchase and use a high-powered air-filtering machine (the type with three types of filter, including the “HEPA”—high efficiency particulate air filter) and leave the machine(s) running constantly so as to keep down the exposure of the child to the airborne allergens almost to zero. This issue is discussed further in Case 1 in Chapter 25, “Weak Constitution.” An asthmatic child will be taking one or more asthma medications. Many will be automatically taking one medicine daily and using additional doses of the same medication or additional medication with the advent of an attack or increased symptoms. Some children (usually with milder conditions) will only take their asthma medication with onset of symptoms, and parents are free to use as needed. It is customary for you NOT to be the person that recommends stopping the medications. First, the prescribing doctor or another doctor consulted should do this, not a non-physician practitioner. Second, it is a courtesy in polite medical practice to refer back to the prescribing physician for a discussion of the issue. It is thus important to consider how an asthmatic child who improves with your treatment may eventually become free of asthma medications. I never recommend stopping. I always recommend the parent return to the prescribing doctor for discussion of how to proceed if the question of medication arises. My experience treating asthmatic children is that after the symptoms start improving, meaning that the asthma attacks appear less often, less strongly, and resolve more easily, and general (between attack) symptoms such as coughing or wheezing improve, the parents start to note the following pattern developing. They report that for the first time they forgot to give their child the daily medication once or twice over the week, with no bad effects. This usually escalates as symptoms continue to improve and over the next weeks they report that they have forgotten to give the automatic medications more often. When the parent either questions what to do with the medication or the child seems spontaneously (with your treatments, of course) not to be remembering to take the medication, I refer the patient back to the referring doctor to check if it is all right that they are doing what they are doing. Usually the doctor is sympathetic to the parents’ interests and encourages them to continue along the same course so long as the symptoms continue to improve, but to always keep the medication(s) to hand should an attack start. Sometimes the doctor does not like this course of action, recommending going back on the daily dose again. This is an issue for the doctor and the patient’s parents to resolve, thus I suggest we continue with treatments and if the condition continues to improve and the medications are spontaneously forgotten again, I eventually refer the parents back to the same doctor again for further discussion. I do not inform parents from the outset to cut back on medications if symptoms improve. I always wait for this to appear spontaneously and without my encouragement. If the parents inquire further on this, I state that we should wait, don’t change anything that is usually done (except specific recommendations such as dietary changes, reducing allergen exposures, giving home treatment). If the treatment is working, it is customary for the medications to start being forgotten. In my opinion we should not encourage this with advice; we should see if it spontaneously occurs. Case 2 Main complaints: Problem with coughing daily for a long time. Over the last several weeks she had a problem with regurgitation and vomiting. History: Like her brother in Case 1 above, this was diagnosed as asthma and she was prescribed an inhaler to be used daily, which she had been using. She had a tendency to catch cold easily, the cold triggering worsening of the asthmatic cough. Diagnosis: From the symptoms and the fact that the right pulse was weaker than the left, I diagnosed lung vacuity pattern. Treatment: I discussed the need to test for sensitivity to cow’s milk products with her mother. Tapping with the herabari was applied to GV-20, GV-12 area, ST-12 area, and LU-1. Stroking with an enshin was applied down the arms, legs, abdomen, back, and neck. Using a teishin, supplementation was applied to LU-9 and SP-5, draining to right LR-3. Press-spheres were left on GV-12 and bilaterally on the “stop coughing” points on the elbows. Second visit—7 days later No symptoms of cough this week. These changes came immediately after treatment. Also her mother discontinued use of the inhaler this week. Treatment: Tapping with the herabari was applied to GV-20, GV-12, ST-12 area, and on the abdomen. Stroking with an enshin was applied down the arms, legs, abdomen, back, and neck. Using a teishin, supplementation was applied to left LU-9 and SP-5, draining to right LR-3. Press-spheres were left on GV-12 and bilaterally on the “stop coughing” points on the elbows. Third visit—5 days later She had a cold over the last few days. She had more vomiting than usual and a problem with diarrhea on this weekend as well. Treatment: Tapping with the herabari was applied to GV-20, ST-12 region, abdomen, LU-1, GV-12, and LI-4. Stroking with an enshin was applied down the arms, legs, back, abdomen, and neck. Using a teishin, supplementation was applied to left LU-9, SP-5, and left GB-37. Press-spheres were left bilaterally on the asthma shu points. Fourth visit—8 days later The cough was much better, but she was still coughing a little in the early morning. The problem of vomiting was unchanged. Treatment: Stroking with an enshin was applied down the arms, legs, back, chest, abdomen, and neck. Using a teishin, supplementation was applied to right KI-7 and LU-5, draining to left SP-9. Press-spheres were left on left BL-20, GV-9, and CV-12.4 __________________ Fifth visit—7 days later The cough was much better; she had almost no symptoms at all. But the problem of vomiting persisted. As the mother described this, Claire threw up on my treatment room floor. Treatment: Tapping with the herabari was applied to PC-6, CV-12, GV-12. Stroking with an enshin was applied down the arms, legs, back, abdomen, chest, and neck. Using a teishin, supplementation was applied to right LU-9 and SP-5, draining to left LR-3. Press-spheres were left on bilateral PC-6 and left BL-20.5 __________________ Sixth visit—13 days later The cough was still better, but had worsened slightly with a cold that started the previous day. The vomiting was a little less frequent. Treatment: Tapping with the herabari was applied on GV-20, GV-12, LI-4, and PC-6. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to right LU-9 and SP-3, draining to left LR-3. Press-spheres were left on bilateral PC-6 and GV-12. Seventh visit—2 weeks later No problem with coughing at all, and her problem with vomiting had also improved significantly—very few episodes during this time. Treatment: Tapping with the herabari was applied to GV-20, GV-12, LI-4, and PC-6. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to right LU-9 and SP-3, draining to left LR-3. Press-spheres were left on GV-12 and bilateral PC-6. Eighth visit—22 days later The coughing remained better and the vomiting had stopped completely. Treatment: Tapping with the herabari was applied to GV-20, GV-12, LI-4, and ST-12 region. Stroking with an enshin was applied down the arms, legs, back, and abdomen. Using a teishin, supplementation was applied to right LU-9 and SP-3, draining to left LR-3. A press-sphere was left on GV-12. Treatment finished as the family moved away. Claire exhibited the same improvements in asthma symptoms as her brother Gilbert from Case 1. The problem she had with regurgitation and vomiting took a little more time but responded well to treatment. Once the asthma symptoms had clearly improved, treatment focused on this secondary problem. Treatment of PC-6 was helpful for the vomiting. If she had not responded with the press-spheres I had thought to replace them with press-tack or intra-dermal needles, but was hesitant because they would be easily within her grasp, which could be dangerous. I did not teach her mother any home treatment as Claire’s condition clearly improved from the first visit.
Asthma
Gilbert, Boy Age 27 Months
 General Approach for Patients with Asthma
General Approach for Patients with Asthma
 Most Likely Pattern-based Root Diagnosis
Most Likely Pattern-based Root Diagnosis
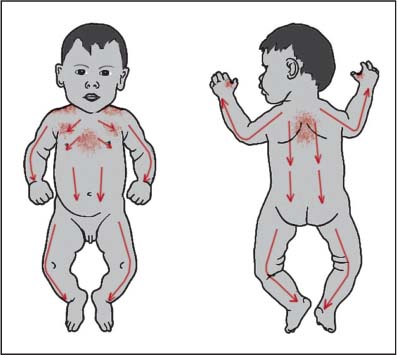
 Typical Non-pattern-based Root Treatment
Typical Non-pattern-based Root Treatment
 Recommendations for Symptomatic Treatment
Recommendations for Symptomatic Treatment
Press-spheres (Ryu), Press-tack Needles (Empishin), and Intra-dermal Needles (Hinaishin)
Needling—the Chishin or Retained Needling Method
Okyu—Direct Moxa
Cupping
Bloodletting
 Other Considerations
Other Considerations
Dietary
Airborne Allergens
Medications
 Further Case Histories
Further Case Histories
Claire, Girl Age 11 Months
Respiratory Problems
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


