CHAPTER 12 RESPIRATORY PATHOLOGY
DEALING WITH THE BIOPSY OR RESECTION SPECIMEN
INDICATIONS FOR REMOVAL OF LUNG TISSUE (Table 12.1)






Table 12.1 Indications for submission of pediatric lung tissue for histopathological examination
| Identification or assessment of primary or secondary neoplasm |
| Assessment of diffuse interstitial lung disease |
| Bronchiectasis |
| Cysts |
| Vascular malformations |
| Assessment of possible infection in immunocompromised patients |
SPECIMEN TYPES
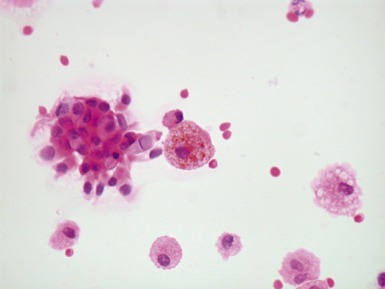
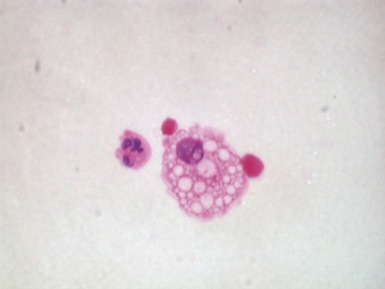
Bronchoalveolar lavage (Columbo et al 1987, ERSTask force 2000)

















Wedge biopsy (Langston et al 2006)














Pneumonectomy








ARTEFACTS, INCIDENTAL FINDINGS AND VARIANTS OF NORMAL
















Fig 12.4 Transbronchial biopsy of lung. The tissue is collapsed and also partly distorted. Assessment of architecture and cellularity is almost impossible on such a specimen.
MALFORMATIONS AND CYSTIC LUNG LESIONS
Introduction




Table 12.2 Cystic lung lesions
| Bronchopulmonary malformations (see Table 12.3) |
| Congenital lobar over inflation |
| Others |
(data from Langston 2003)
Table 12.3 Bronchopulmonary malformations
Bronchial atresia with connection to the gastrointestinal tract (intralobar sequestration/complex or communicating bronchopulmonary foregut malformation) |
(data from Langston 2003)
Classification
Table 12.4 Congenital pulmonary airway malformation (CPAM)
| Type 0 | acinar dysgenesis/dysplasia |
| Type 1 | large cyst type |
| Type 2 | small cyst type |
| Type 3 | adenomatoid type |
| Type 4 | peripheral type |
(data from Stocker 2002)
CONGENITAL PULMONARY AIRWAY MALFORMATION

















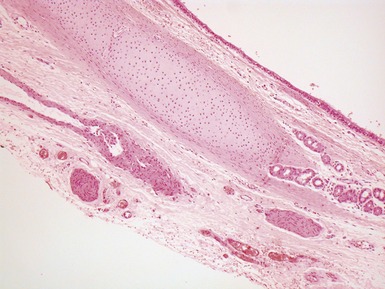
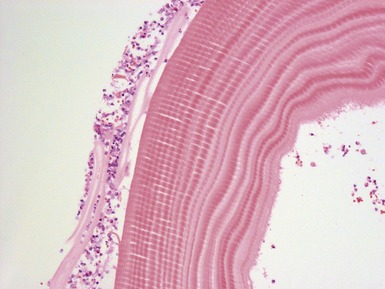
 lined by ciliated, pseudostratified columnar epithelium with wall of fibromuscular tissue and cartilage (Fig 12.13)
lined by ciliated, pseudostratified columnar epithelium with wall of fibromuscular tissue and cartilage (Fig 12.13)




















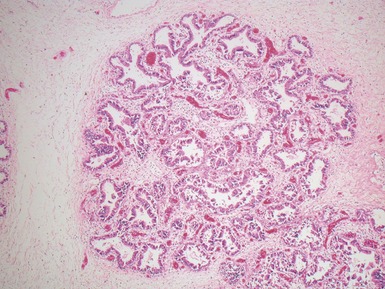
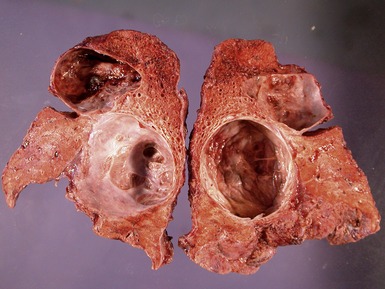
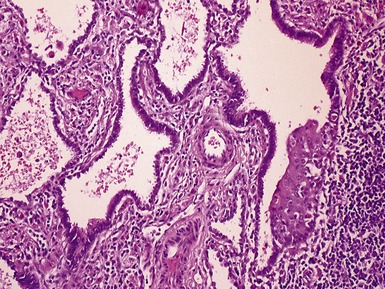
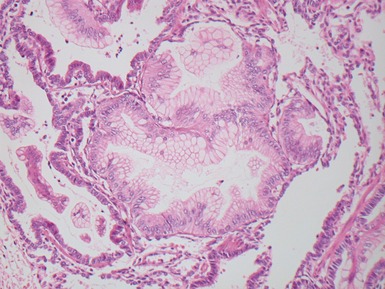
Fig 12.14 CPAM type 1. One-month-old baby girl with cystic lesion in left lower lobe of lung. The excised lobe showed obvious cysts, the largest 1.8cm in diameter. The lining of the cysts resembles that in Fig 12.13 but, in addition, there are areas of mucin-secreting epithelium, with a resemblance to gastric epithelium. Some smooth muscle is evident in the cyst walls.

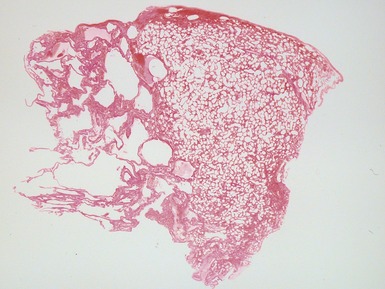
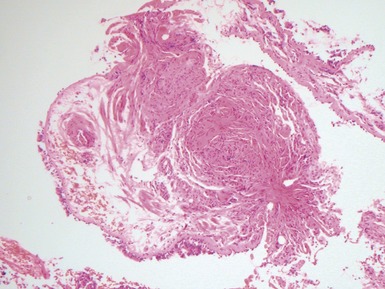
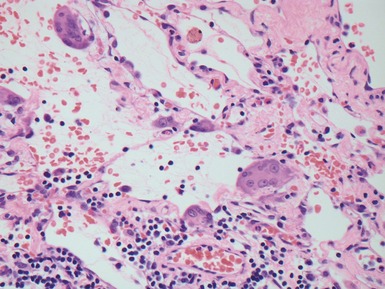
Fig 12.16 CPAM type 2. Same case as Fig 12.15. A low power view of a section from junction of normal and cystic lung. The multiple small cysts with thin walls are well appreciated as is the relatively well-defined border of the lesion. (H&E)
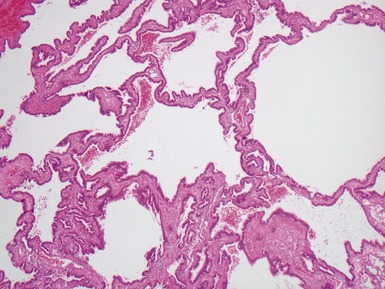
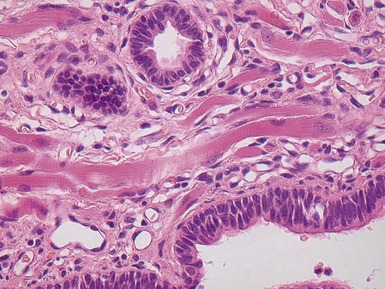
Fig 12.18 CPAM type 2. Striated muscle fibers run through the stroma of the cyst walls; so-called rhadomyomatous dysplasia. Rhabdomyomatous dysplasia may also be seen in other abnormal lungs such as in pulmonary hypoplasia with or without diaphragmatic hernia and may be focal or diffuse throughout the lung parenchyma. The origin of the skeletal muscle is not known. It may represent ingrowth from adjacent structures such as esophagus, but equally it may represent differentiation of pulmonary mesenchyme.
BRONCHIAL ATRESIA



EXTRALOBAR SEQUESTRATION

Histopathological features



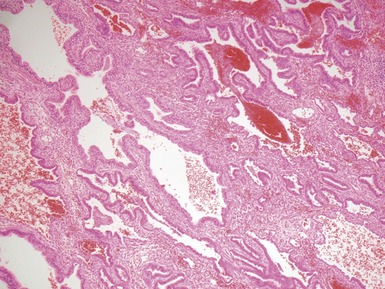
Fig 12.21 Extralobar sequestration. Photomicrograph of the same specimen as Fig 12.20. The lung shows cystic change resembling CPAM type 2. There is some fresh traumatic hemorrhage. There was also chronic inflammation. It contained striated muscle fibers. Cartilage-containing bronchi were also present.
INTRALOBAR SEQUESTRATION
Histopathological features





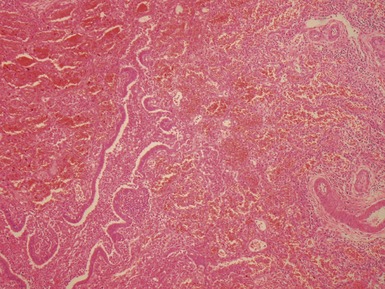
Fig 12.23 Intralobar sequestration. Photomicrograph of specimen Fig 12.22. There is extensive fresh hemorrhage and there is active inflammation. The bronchi and bronchioles are distended by purulent material. The arteries appear thick-walled.
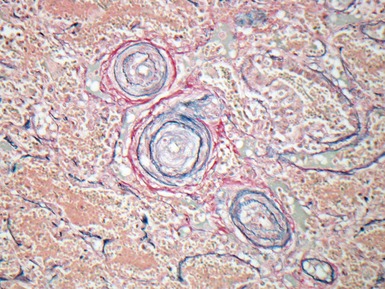
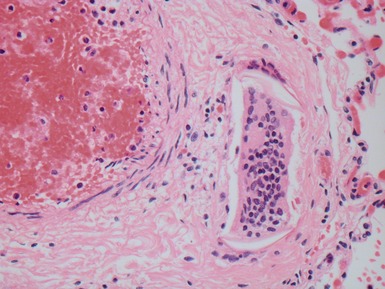
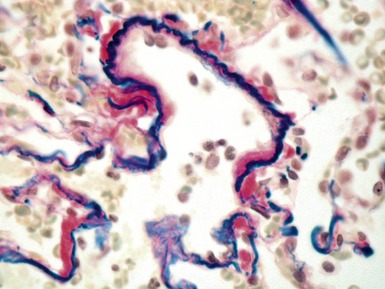
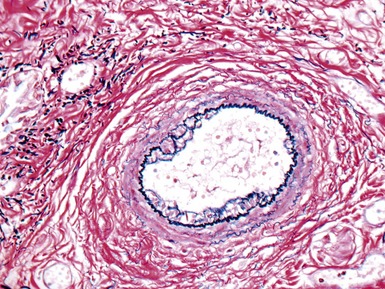
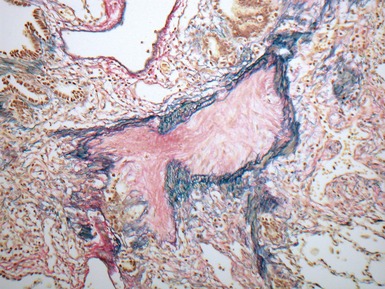
Fig 12.24 Intralobar sequestration. Photomicrograph of the peripheral vasculature in the same case as Figs 12.22 and 12.23. There is muscularization of the intra-acinar arteries and there is also intimal cellular proliferation, both features indicating pulmonary arterial hypertension, presumably from exposure to the systemic arterial pressure of the anomalous systemic arterial supply. (EVG)

LOBAR EMPHYSEMA
Congenital lobar overinflation




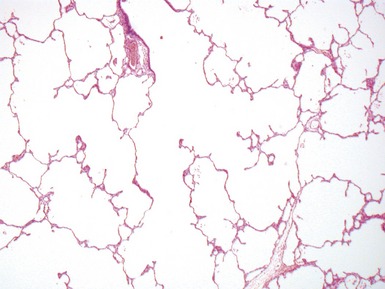
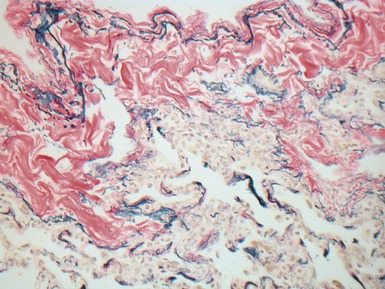
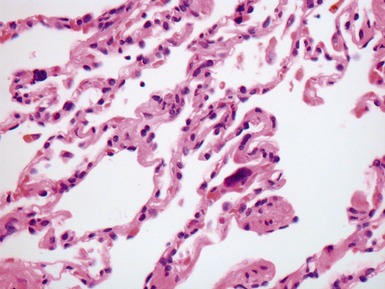
Fig 12.26 Congenital lobar overinflation. Photomicrograph from specimen in Fig 12.25. There is overdistension of alveoli and alveolar ducts (to four to five times the normal diameter). The magnitude of the distension may not be evident until compared with an age-matched control section of lung. Interstitial emphysema was also evident but no other abnormality. No bronchial obstruction could be demonstrated. (H&E)


BRONCHOGENIC CYST







HYDATID CYST









INTERSTITIAL LUNG DISEASE




Classification


Table 12.5 North American classification of diffuse lung disease in children under 2 years
(data from Deutsch et al 2007)
CONGENITAL SURFACTANT DEFICIENCY












