CHAPTER 1 RENAL PATHOLOGY
INTRODUCTION








PEDIATRIC RENAL TUMORS
OVERVIEW



 in the United Kingdom, diagnostic percutaneous needle biopsy is usually performed for initial diagnosis prior to commencement of chemotherapy and nephrectomy carried out following chemotherapy
in the United Kingdom, diagnostic percutaneous needle biopsy is usually performed for initial diagnosis prior to commencement of chemotherapy and nephrectomy carried out following chemotherapy

WILMS’ TUMOR / NEPHROBLASTOMA

Table 1.1 Syndromic associations of Wilms’ tumor
| Wilms’ aniridia genital anomaly retardation (WAGR) syndrome |
| Beckwith–Wiedemann syndrome |
| Hemihypertrophy |
| Denys–Drash syndrome |
| Familial nephroblastoma |
| Frasier syndrome |
| Simpson–Golabi–Behmel syndrome |
| Neurofibromatosis |
| Perlman syndrome |
Epidemiology





Genetics

Clinical features




Specific issues of specimen handling



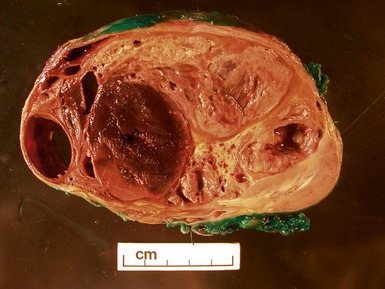
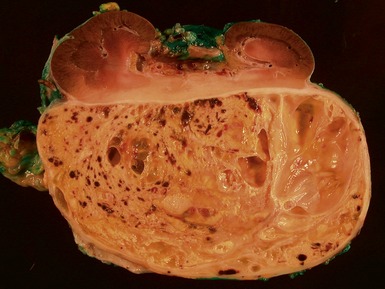
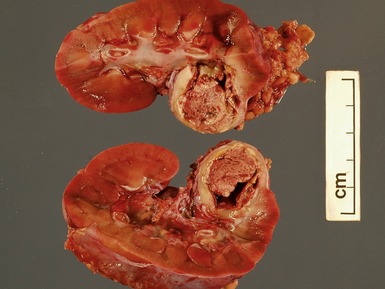
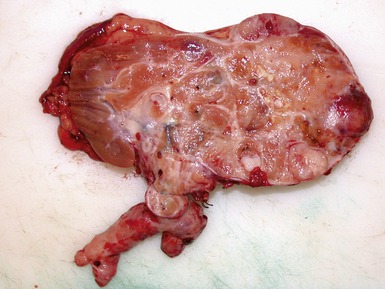
Macroscopic features (Figs 1.1–1.7)







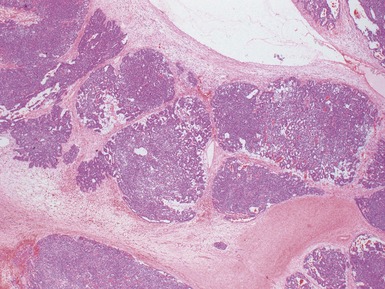
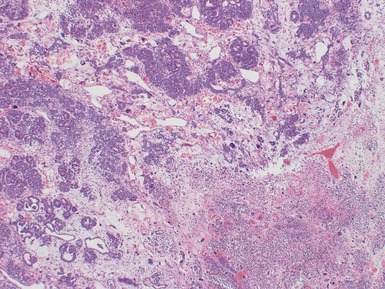
Histopathological features






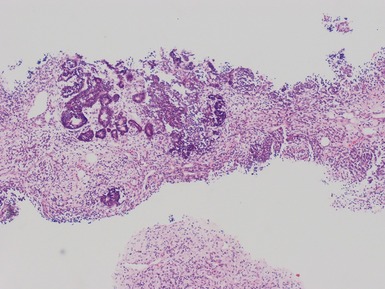
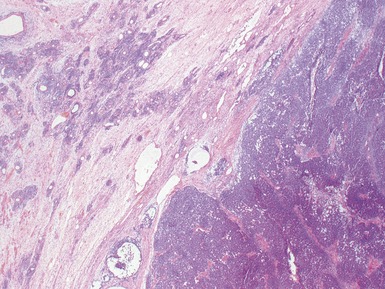
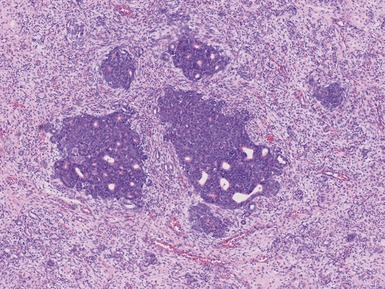
Figs 1.13–1.14 Photomicrographs of nephroblastomas showing the classical architectural and morphological mixture of elements.
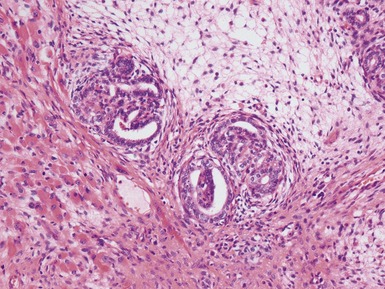
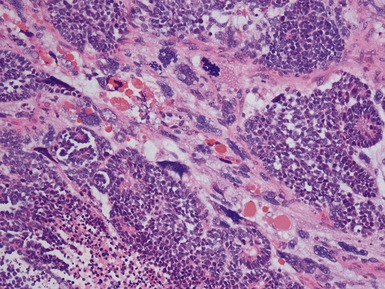
Epithelial component (Figs 1.15–1.18)

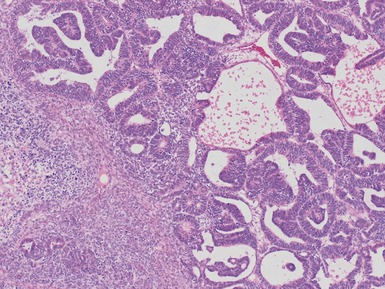
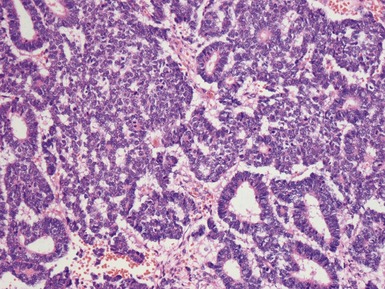
Figs 1.15–1.16 Photomicrographs of nephroblastomas showing epithelial elements manifest as well-formed tubular structures.
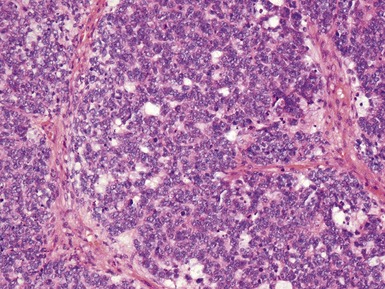
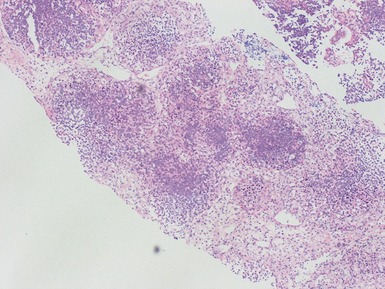
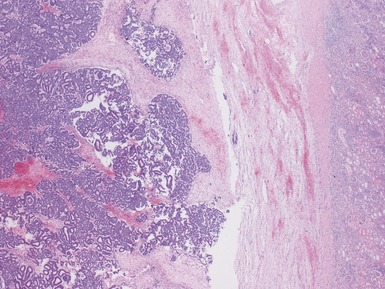
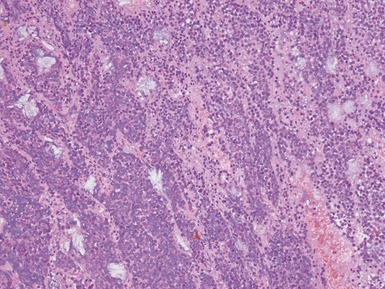
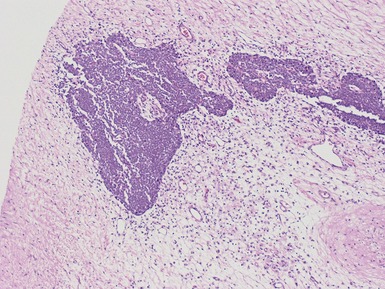
Blastemal component (Figs 1.19–1.21)








Figs 1.19–1.20 Photomicrographs of nephroblastomas showing blastemal areas admixed with other elements.
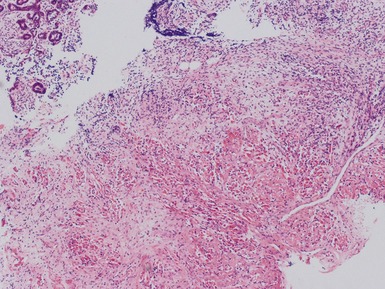
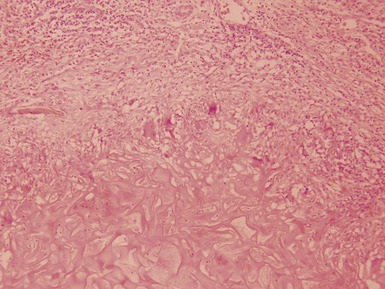
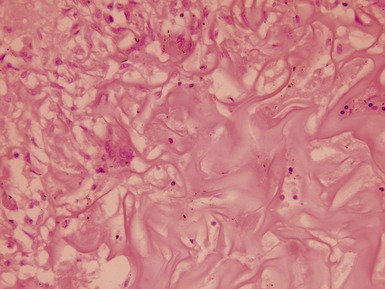
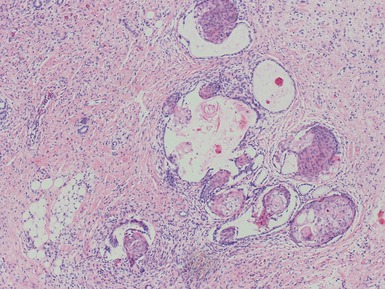
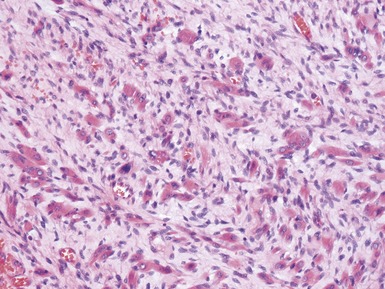
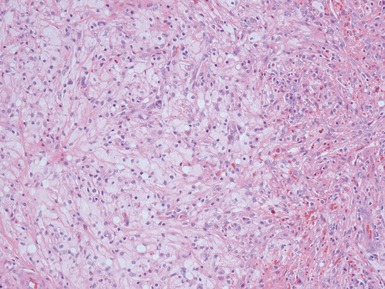
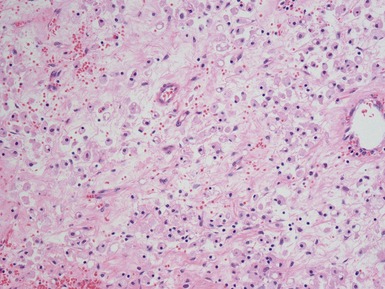
Stromal component (Figs 1.22–1.25)
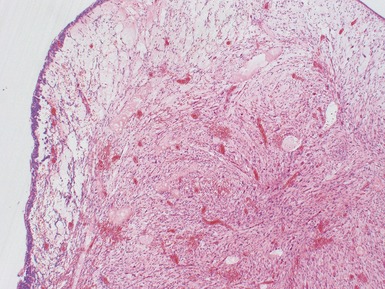
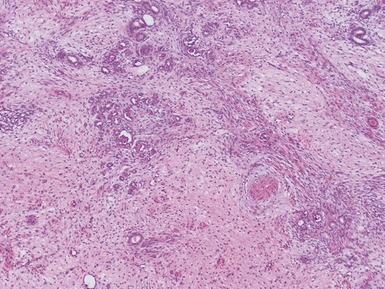
Figs 1.22–1.24 Photomicrographs of nephroblastomas showing predominant stromal differentiation admixed with other elements.
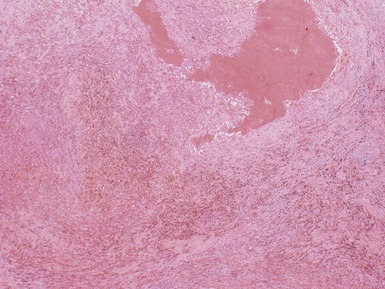
Post-chemotherapy features (Figs 1.26–1.30)







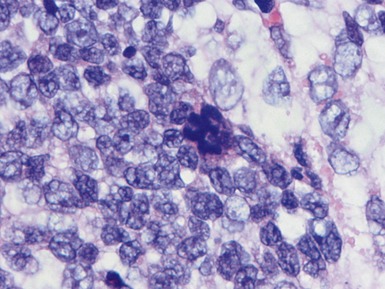
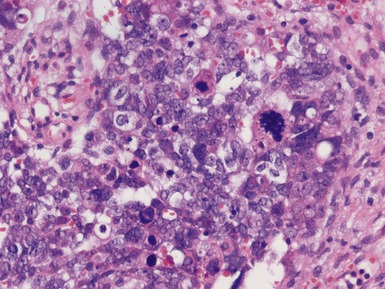
Unfavorable histology Wilms’ tumor (anaplasia) (Figs 1.31–1.34)














 recently suggested that there may be a gene expression signature for relapse of primary Wilms’ tumors independent of anaplasia (Li et al 2005a)
recently suggested that there may be a gene expression signature for relapse of primary Wilms’ tumors independent of anaplasia (Li et al 2005a)

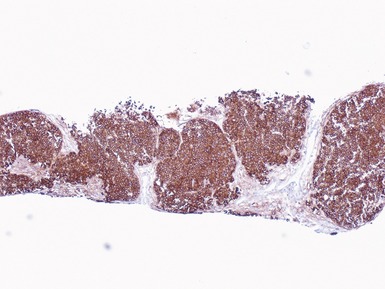
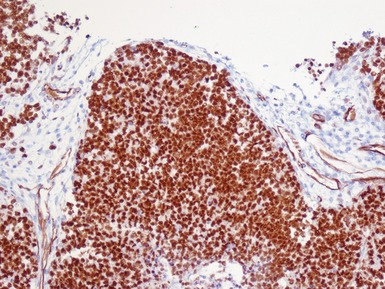
Immunohistochemical staining


Classification and staging
Table 1.2 SIOP Classification (Vujanic et al 2002)
| A. Pre-treated cases | Low risk | Mesoblastic nephroma |
| Cystic partially differentiated nephroblastoma | ||
| Completely necrotic nephroblastoma | ||
| Intermediate risk | Nephroblastoma – epithelial type | |
| Nephroblastoma – stromal type | ||
| Nephroblastoma – mixed type | ||
| Nephroblastoma – regressive type | ||
| Nephroblastoma – focal anaplasia type | ||
| High risk | Nephroblastoma – blastemal type | |
| Nephroblastoma – diffuse anaplasia | ||
| Clear cell sarcoma of the kidney | ||
| Rhabdoid tumor of the kidney | ||
| B. Primary nephrectomy cases | Low risk | Mesoblastic nephromaCystic partially differentiated nephroblastoma |
| Intermediate risk | Non-anaplastic nephroblastoma and its variants | |
| Nephroblastoma – focal anaplasia | ||
| High risk | Nephroblastoma – diffuse anaplasia | |
| Clear cell sarcoma of the kidney | ||
| Rhabdoid tumor of the kidney |
If necrosis and regressive change comprises more than two-thirds of the tumor mass it is a regressive type.
If regressive change / necrosis comprises less than two-thirds of the tumor mass a predominant histological component should be looked for and the tumor subclassified accordingly.
For a component to be regarded as dominant, more than two-thirds of the viable tumor must be composed of the subtype.
If >10% and <66% of the viable tumor is blastema, mixed type regardless of ‘dominant’ component.
To fulfill the diagnosis for completely necrotic subtype there must be no viable tumor present on gross and microscopic examination of multiple blocks from different areas of the tumor sampled at least one block per centimeter of tumor largest diameter, in combination with the presence of regressive and necrotic changes caused by chemotherapy.
Table 1.3 Staging system: SIOP
| Stage I | a.The tumor is limited to kidney or surrounded with a fibrous pseudocapsule if outside of the normal contours of the kidney. The renal capsule or pseudocapsule may be infiltrated with tumor but it does not reach the outer surface, and is completely resected (resection margins clear) |
| b.The tumor may be bulging into the pelvic system and dipping into the ureter but not infiltrating their walls | |
| c.The vessels of the renal sinus are not involved | |
| d.Intrarenal vessel involvement may be present | |
| Fine needle aspiration or percutaneous cord needle biopsy does not upstage the tumor | |
| The presence of necrotic tumor or chemotherapy-induced change in the renal sinus and/or within the perirenal fat should not be regarded as a reason for upstaging a tumor providing it is completely excised and does not reach the resection margins | |
| Stage II | a.The tumor extends beyond the kidney or penetrates through the renal capsule and/or fibrous pseudocapsule into perirenal fat but is completely resected (resection margins clear) |
| b.Tumor infiltrates the renal sinus and/or blood and/or lymphatic vessels outside the renal parenchyma but is completely resected | |
| c.Tumor infiltrates adjacent organs or vena cava but is completely resected | |
| Stage III | a.Incomplete excision of the tumor which extends beyond resection margins (gross or microscopical tumor remains postoperatively) |
| b.Any abdominal lymph nodes are involved | |
| c.Tumor rupture before or intraoperatively | |
| d.The tumor has penetrated through the peritoneal surface | |
| e.Tumor implants are found on the peritoneal surface | |
| f.Tumor thrombi present at resection margins of vessels or ureter, transected or removed piecemeal by surgeon | |
| g.The tumor has been surgically biopsied (wedge biopsy) prior to preoperative chemotherapy or surgery | |
| The presence of necrotic tumor or chemotherapy-induced changes in a lymph node or at the resection margins is regarded as proof of previous tumor with microscopic residue and therefore the tumor is assigned stage III because of the possibility that some viable tumor is left behind in the adjacent lymph node or beyond resection margins | |
| Stage IV | Hematogenous metastasis or lymph node metastasis outside the abdominal and pelvic region |
| Stage V | Bilateral renal tumors at diagnosis. Each side should be sub staged according to the above classification |
| Stage I | Limited to kidney and completely resected, renal capsule intact |
| Fine needle aspiration or percutaneous core needle biopsy does not upstage the tumor | |
| The presence of necrotic tumor or chemotherapy-induced change in the renal sinus and/or within perirenal fat should not be regarded as a reason for upstaging a tumor providing it is completely excised and does not reach the resection margins | |
| Stage II | Tumor infiltrates beyond kidney but is completely resected |
| a.The tumor extends beyond the kidney or penetrates through the renal capsule and/or fibrous pseudocapsule into perirenal fat but is completely resected (resection margins clear) | |
| b.Tumor infiltrates the renal sinus and/or blood and/or lymphatic vessels outside the renal parenchyma but is completely resected | |
| c.Tumor infiltrates adjacent organs or ureter but is completely resected | |
| Stage III | Gross or microscopic residual tumor confined to abdomen |
| a.Incomplete excision of the tumor which extends beyond resection margins (gross or microscopical tumor remains postoperatively) | |
| b.Any abdominal lymph nodes are involved | |
| c.Tumor rupture before or intraoperatively | |
| d.The tumor has penetrated through the peritoneal surface | |
| e.Tumor implants are found on the peritoneal surface | |
| f.Tumor thrombi present at resection margins of vessels or ureter, transected or removed piecemeal by surgeon | |
| g.The tumor has been surgically biopsied (wedge biopsy) prior to preoperative chemotherapy or surgery | |
| Stage IV | Hematogenous metastasis or lymph node metastasis outside the abdominal and pelvic region |
| Stage V | Bilateral renal tumors at diagnosis. Each side should be sub staged according to the above classification |
Special diagnostic investigations
Differential diagnoses and pitfalls







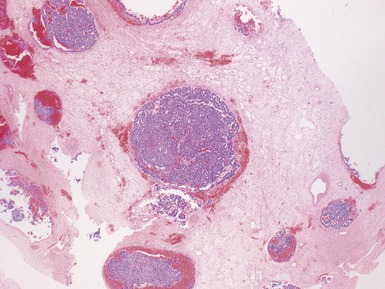
 occasionally there may also be marked accumulation of Tamm–Horsfall protein within the subcapsular sinus (Fig 1.40)
occasionally there may also be marked accumulation of Tamm–Horsfall protein within the subcapsular sinus (Fig 1.40)
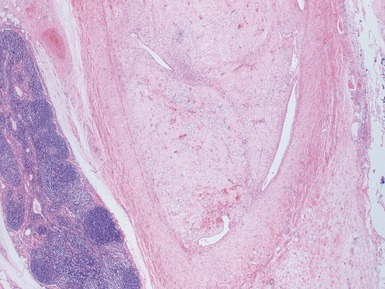
Fig 1.37 Photomicrograph showing involvement of hilar renal vein branch by postchemotherapy nephroblastoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


