Fig. 19.1
Compression view of the right lower quadrant from SBFT demonstrates a long segment of narrowed, ulcerated and nodular appearing ileum giving the characteristic “cobblestone” appearance (arrows). Loop separation caused by thickening of bowel walls and mesentery inflammation
Early changes of CD include aphthous lesions, a coarse granular pattern, nodularity, and fold thickening, which may progress to deeper ulceration, cobblestoning, and fissuring. In the colon, ulceration occurs within a background of normal-appearing mucosa. Inflammatory edema produces mucosal elevations seen more commonly in the colon than the small bowel. In the patient with more severe CD, mucosal distortions and pseudopolyps may occur due to the elevation of submucosa at the margins of healing ulcers. As inflammation spreads in transmural and circumferential dimensions, the radiologic findings progress to strictures and shortening, with the most severe cases producing the characteristic “string sign.” In addition, bowel may be noted to adhere to adjacent loops or to other viscera and deep ulcers may extend to create fistula. The finding of discontinuous, patchy, and asymmetric colonic mucosal changes is a hallmark of CD.
Contrast studies are limited in their ability to image extraluminal extension of disease or extraintestinal manifestations. Only indirect assessment of bowel wall thickening or mesenteric involvement can be made. Mesenteric inflammation, thickening, and fibrosis may cause separation and shortening of bowel loops. Mesenteric lymphadenopathy may appear as extraluminal masses indenting the bowel wall.
Computer Tomography
Computer tomography (CT) still is the most widely used cross-sectional imaging modality in patients with CD given its wide availability. Its major role in children with CD is in the evaluation of disease extent and in assessing for complications, particularly in the acute situation. CT enteroclysis has been shown to be more accurate than SBFT in the diagnosis of CD, but neither is able to detect the early mucosal changes of CD [2]. Additionally, as with any enteroclysis study, this technique requires the introduction of a nasojejunal tube, generally not well accepted in the pediatric population. Changes readily detected by CT include bowel wall thickening, luminal narrowing, and mesenteric involvement. Mesenteric findings include thickening due to fibrofatty infiltration, lymphadenopathy, and fatty encroachment of the affected loop of bowel.
Patients with known CD, who present with new acute symptoms suspicious for complications or a deteriorating clinical course, are best imaged with CT to assess for progressive disease or the onset of complications such as obstruction, fistulae, abscesses, or malignant change (Fig. 19.2). Extraintestinal manifestations of CD in the hepatobiliary, pancreatic, urinary, and musculoskeletal systems are also readily assessed by CT. Specific CT findings of complications and extraintestinal manifestations of CD are discussed below.
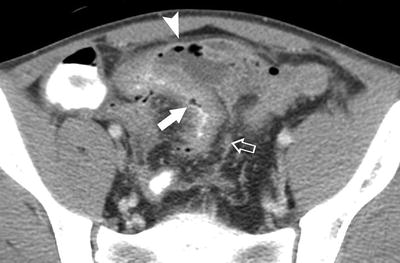
Fig. 19.2
Oral and intravenous contrast enhanced CT image of the pelvis. A thickened loop of small bowel containing intraluminal contrast (white arrow) marginates an intra-abdominal abscess containing fluid and air (arrow head). An enhancing fistulous tract is seen extending to the base of the abscess cavity (open arrow)
The sensitivity of CT scan in patients with CD is increased by optimal opacification and distension of the bowel by administering oral contrast at an age- and weight-appropriate dose, or by the enteroclysis technique. Bowel wall thickening greater than 3 mm in pediatric patients is generally considered abnormal [3]. Given that this young patient population frequently undergoes multiple studies, the current trend is moving toward MRI evaluation in the non-acute setting, thus minimizing exposure to ionizing radiation.
Magnetic Resonance Imaging
MRI offers unique advantages to the pediatric patient because, in addition to being noninvasive, it avoids exposure to ionizing radiation. In many cases, MRI can replace or complement CT because its excellent soft tissue contrast and three-dimensional capabilities are ideal properties for imaging the bowel [4]. In the past, motion artifacts often limited MRI, but this problem has been largely overcome by the recent introduction of respiration-suspended sequences. Other technological advances, including improved coils, fat suppression, use of oral agents and intravenous gadolinium, powerful gradient systems, and ultrafast pulse sequences have led to overall improvement in gastrointestinal imaging. Optimal image quality depends greatly on adequate luminal distension with contrast medium. Without enteric contrast, MRI has produced inconsistent results in children with CD [5, 6].
The method of enteric contrast administration has proved to be a critical factor because oral ingestion of contrast agents that do not provide adequate bowel distention such as routine positive contrast agents or water, while patient-friendly, produces inadequate luminal distension, downgrades the image quality, and may limit the ability to detect early or minimal disease. The two techniques found to have the greatest success to evaluate for CD of the small bowel include MR enteroclysis and MR enterography utilizing a negative contrast agent that provides adequate bowel distention. The choice of oral contrast agent for MR enterography varies with institution. However, at our institution, we utilize VoLumen, a low-concentration barium (0.1% weight/volume) that contains sorbitol to aid in bowel distention.
Magnetic resonance enteroclysis requires duodenal intubation to permit volume challenge, which causes reflex bowel atony and produces superb contrast for evaluating luminal, transmural, and extramural changes. It has been postulated that by combining the advantages of enteroclysis with three-dimensional cross-sectional imaging, MR enteroclysis has been touted as the only imaging modality that can provide comprehensive diagnostic information on small bowel CD [4]. However, routine use of MR enteroclysis in children has not been widely adopted because of the need to insert a duodenal tube fluoroscopically, entailing exposure to ionizing radiation and, the potential need for intravenous sedation.
Prospective comparison of MR enterography and CT enterography in the evaluation of small bowel CD has been performed [7] with the sensitivities for detecting active small bowel disease found to be similar (90.5% vs. 95.2%, respectively). Although MR enterography had a slightly lower sensitivity and specificity, this difference was not statistically significant for the 30 patients who underwent both imaging studies. However, image quality across the study cohort was better with CT enterography. In another study [8], MR enterography demonstrated good sensitivity in the detection of active CD and found good correlation between MR and CT enterography in the evaluation of wall thickening with mucosal hyperenhancement and the presence of the comb and halo signs. While CT enterography was found to be superior in the detection of fibrofatty proliferation and mesenteric lymph nodes, MR enterography was superior in the evaluation of fistulas. Currently, however, because MR enterography has a diagnostic effectiveness comparable to that of CT enterography [9], the trend is increasing toward MR enterography as a radiation-free alternative for the evaluation of patients with CD. Indeed, one study [10] concluded that MR enterography can be substituted for CT as the first-line imaging modality in pediatric patients with CD. This viewpoint is based on the ability of MR enterography to detect intestinal pathologic abnormalities in both small and large bowel as well as extraintestinal disease manifestations. Furthermore, MR enterography provides an accurate noninvasive assessment of CD activity and mural fibrosis and can aid in formulating treatment strategies for symptomatic patients and assessing therapy response [10].
The technique for MR enterography begins with the oral ingestion of contrast, but the type of oral contrast used again is controversial and is usually institution-specific. Again, at our institution the utilization of VoLumen, low-concentration barium that contains sorbitol to aid in bowel distention, has been well tolerated and shown to produce good quality images. The patient is asked to ingest three 450 mL bottles over approximately 1–1½ h as tolerated, with each bottle being ingested over approximately 20 min. The field of view includes the abdomen and majority of the pelvis to evaluate the entirety of the small bowel. Imaging of the bowel begins with coronal T2 single-shot fast-spin echo imaging, which is reviewed by the radiologist to ensure adequate oral preparation with contrast reaching the colon. If adequate, the remainder of the MR enterography protocol is performed including axial T2-weighted axial diffusion-weighted sequence to evaluate for restricted diffusion in areas of pathologic edema, coronal pre-gadolinium T1-weighted, and dynamic steady-state free precession imaging in the coronal plane to evaluate for bowel peristalsis. The evaluation is enhanced utilizing intravenous glucagon to inhibit bowel motion in preparation for the longer post-gadolinium sequences following the administration of IV contrast. These include axial, coronal, and sagittal T1-weighted sequences to evaluate enhancement pattern. MR findings of active CD affecting the small bowel include mucosal hyper enhancement, wall thickening (Fig. 19.3a, b), restricted diffusion (Fig. 19.4), ulcers, mesenteric hypervascularity (Comb sign, Fig. 19.5), mesenteric inflammation, and reactive mesenteric nodes. Fibrostenotic lesions (Fig. 19.6a, b) may show homogenous T2 hyperintensity, uniform contrast enhancement, and minimal adjacent inflammatory changes. Complications of CD include penetrating disease and bowel obstruction, sinus tracts, fistulas, and abscess formation [11].
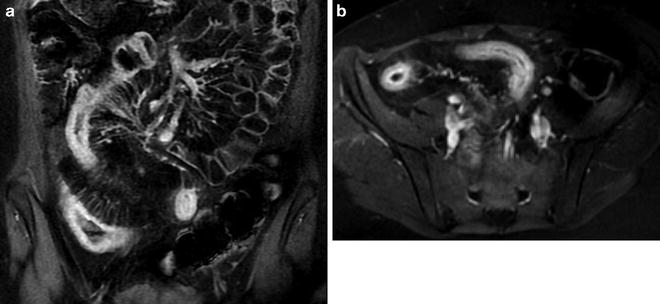
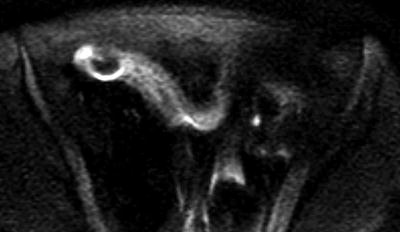

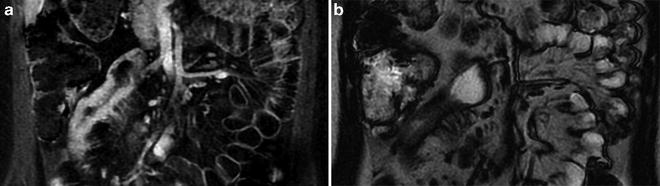
Fig. 19.3
Coronal (a) and axial (b) post-gadolinium T1-weighted sequences illustrating mucosal hyper enhancement and wall thickening along a segment of bowel with active inflammation
Fig. 19.4
Axial diffusion-weighted sequence demonstrates an area of restricted diffusion consistent with pathologic edema along a segment of affected bowel
Fig. 19.5
Coronal post-gadolinium T1-weighted sequence demonstrates mesenteric hypervascularity consistent with prominent vasa recta subtending a segment of affected bowel (Comb sign)
Fig. 19.6
Coronal post-gadolinium T1-weighted sequence revealing a fibrostenotic lesion showing homogenous T2 hyperintensity, uniform contrast enhancement, and minimal adjacent inflammatory changes. Dynamic sequences (not shown) showed non-peristalsis along this involved segment
In addition to MR enterography in the assessment of IBD, we currently also use MRI of the pelvis for the evaluation of complex perianal disease, as discussed below.
Ultrasound
The lack of ionizing radiation and noninvasive nature of US make it an ideal method of evaluation in children. In addition, for routine US imaging, bowel cleansing is not required, nor is enteric or intravenous contrast. However, because it is operator dependent, its role in patients with CD is currently generally limited to the evaluation of complications, particularly abscesses, and extraintestinal disease manifestations. It is rarely used for primary diagnosis. Affected bowel segments demonstrate wall thickening, lack of peristalsis, and poor stratification of the different layers (Fig. 19.7a) [12]. Similar to adults, US findings in children with CD show good correlation with endoscopy [13]. The most promising use of US may be in the ongoing evaluation of disease activity as well as response to treatment. In children, the sonographic value of bowel wall thickening as an index of increased disease activity has been demonstrated [14, 15]. With moderate–severe disease, the predictive value of increased bowel wall thickening greater than 2.5 mm in the ileum as an index of active disease was 88% (82% for colon >3 mm) [14]. Assessment of disease severity can also be enhanced by measuring the vessel density in the affected bowel segment using color Doppler US (Fig. 19.7b) [16]. When incorporated into a clinical protocol, US may reduce the need for contrast studies [14, 17]. In expert hands, US has been used to assess fistulae and strictures, and also monitor postoperative disease recurrence [18].
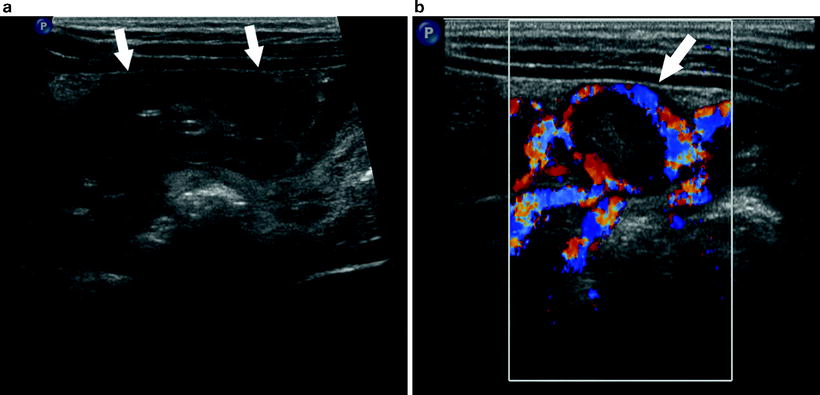
Fig. 19.7
(a) Longitudinal ultrasound of the right lower quadrant demonstrates a segmental region of thickened, hypoechoic small bowel (arrows). (b) Transverse Doppler image demonstrates hyperemia of bowel wall (arrow)
There are a number of limitations to the use of US in CD. Although the assessment of terminal ileal disease with US is quite good, the proximal small bowel and distal portions of the colon are poorly imaged. In addition, superficial lesions as seen in early disease can be missed in both children and adults [13].
Ulcerative Colitis
Ulcerative colitis is a chronic, idiopathic, inflammatory disease of the rectal and colonic mucosa that is characterized by mucosal inflammation, edema, and ulceration. Several distinguishing features permit clinical and radiological distinction from CD. As a rule, UC nearly always affects the rectum and extends proximally to involve a variable length of colon in a contiguous fashion. Other than the occasional “backwash ileitis” of the terminal ileum, the small bowel is not affected. On rare occasions, variants with transmural involvement or without rectal inflammation also occur. Radiologic features of UC are quite distinct, although in the majority of cases, diagnosis is dependent on clinical presentation, laboratory tests, and findings on colonoscopy and biopsy.
Imaging Techniques
Plain Radiographs
The nonspecific finding of mucosal edema occasionally noted on plain films is rarely helpful for diagnosis. However, in the patient presenting acutely with symptoms of toxic megacolon, the plain film shows marked colon dilatation and is adequate for monitoring response to treatment and the potential onset of bowel perforation.
Contrast Enema
Given the availability of colonoscopy and its ability to obtain tissue for histologic assessment, as well as the discomfort of BE, contrast studies of the colon are less commonly performed than in the past. However, if needed, it can be used for confirming the diagnosis, evaluating extent and severity of disease, and detecting complications. The earliest change seen on the air-contrast study is a fine granular pattern of the colonic mucosa, which may be associated with blunting and broadening of the haustral folds due to mucosal edema. As the disease progresses, mucosal irregularity increases (Fig. 19.8). Subsequently, ulcers appear and begin to extend deeper, undermining the submucosa and forming flask-shaped or “collar-button” ulcers. Extensive mucosal ulceration may leave islands of residual inflamed mucosa that are recognized as “inflammatory pseudopolyps.” In contrast to CD, these changes are contiguous, circumferential, and symmetric with no skip lesions. With long-standing disease, the colonic wall becomes rigid, shortened, and narrow due to fibrosis of the submucosa, giving the appearance of the “lead pipe” colon.
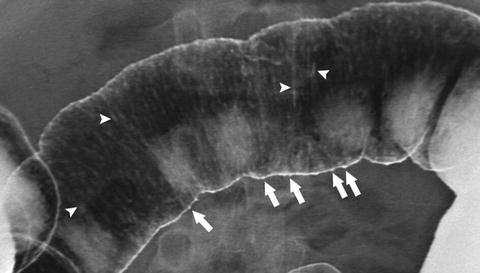
Fig. 19.8
Image (ACBE–UC). Anterior image of the transverse colon from ACBE demonstrating granular mucosa with early ulcerations seen in profile (arrows) and en face (arrow heads)
A contrast enema should be administered with extreme caution in the patient with an acute presentation. A physical examination to exclude peritoneal signs and a plain film to rule out toxic megacolon and free air should be performed prior to a BE, as any of these findings would be a contraindication.
CT
CT may be useful in differentiating UC from CD, and it has the advantage of being able to visualize bowel wall as well as adjacent structures [19]. Adequate preparation for the CT examination is important. When optimal colonic imaging is desired, oral contrast should be given sufficient time to opacify the entire small bowel and colon, and if necessary additional rectal contrast should be administered. Early mucosal changes are difficult to detect on CT, but in chronic disease, bowel wall thickening and luminal narrowing is readily seen [20]. However, these rather nonspecific findings overlap with those of other colitides including Crohn colitis [19, 21]. Characteristic CT features in UC include a symmetric, contiguous wall thickening involving the rectum and extending proximally in a contiguous manner. Small bowel changes and skip lesions are absent. Thickening of the mesentery or mesenteric lymphadenopathy are rare, but proliferation of perirectal fat can occur.
MRI
Characteristic findings of MRI in the active stage of UC include loss of haustral markings, thickening, and contrast enhancement of the colonic wall [22, 23]. As with CT, these findings overlap those of CD. The few early pediatric studies available reveal inconsistencies in the ability of MRI to differentiate UC from CD [5, 6]. However, a diagnosis of UC was supported when disease progressed from the rectum proximally with mucosal enhancement and a low-signal submucosal stripe [5].
Recent advances in contrast-enhanced MRI among the pediatric population indicate that gadolinium-enhanced-MRI favorably compares with endoscopy as a means to differentiate between CD and UC. However, endoscopy has the clear advantage in allowing tissue samples to be obtained for histologic evaluation, and thus cannot yet be replaced by MRI [6]. While MRI can detect the presence of colonic disease, at present, it seems more promising for characterizing small bowel disease related to IBD. Also, the ability of MRI to categorize disease into either CD or UC with high specificity remains a challenge.
US
As previously noted, US has the advantages of being cheap, noninvasive, and lacking in ionizing radiation, but its principal finding of increased bowel wall thickness is nonspecific and cannot distinguish between UC and CD. In addition, early mucosal changes are not detected with US and the difficulty in visualizing the rectosigmoid limits its ability to evaluate the true extent of the disease. In the few pediatric studies, there appears to be a consensus that the appropriate role of US is in the monitoring of disease activity and assessing response to treatment [14, 24, 25]. With moderate–-severe disease, the predictive value of increased bowel wall thickening greater than 3 mm in the colon as an index of active disease was 82% [14].
Indeterminate Colitis
Patients with IBD whose clinical, endoscopic, pathologic, and radiologic presentation cannot easily be differentiated into CD or UC are assigned the diagnosis of indeterminate colitis (IC). Indeterminate colitis appear to be more common in children compared to adults, with a prevalence rate of nearly 30% recently reported in a cohort of 250 children with IBD [26].
One study has shown that the probability of making a definitive diagnosis of either CD or UC increases with age [11]. Careful radiologic evaluation may play a significant role in subsequent reclassification of patients with IC. The distinction between CD and UC may be important in selecting appropriate treatment and in determining prognosis.
Demonstration of small bowel inflammation, skip lesions, and mesenteric extension usually indicates CD, particularly in the absence of colonic disease. Patients classified as IC usually have normal small bowel imaging on the SBFT and CT. As noted previously, newer techniques such as US, radionuclide scans, and MRI may demonstrate small bowel disease, particularly in the distal ileum. Again, MR enterography is becoming a promising technique and with recent advances in imaging, the detection of IBD has improved for both small bowel and colonic disease. However, in isolated colonic disease, the ability to distinguish UC and CD with high specificity remains a challenge. When extensive colonic disease is present, the finding of terminal ileal inflammation may be misleading because some patients with UC may have “backwash ileitis.”
Although the colon is usually accessible for endoscopic evaluation, cross-sectional imaging with CT or MRI may demonstrate transmural involvement, extension into mesenteric fat, fistulae, or abscesses, which may prompt a more definitive reclassification as CD. Using US to differentiate between CD and UC have so far proved unreliable in children, although it may be useful for monitoring disease activity [13, 15, 27].
Other Radiologic Modalities in IBD
White Blood Cell Scan
Radionuclide-labeled autologous White Blood Cell (WBC) reinjected intravenously are taken up by inflamed tissues and can then be detected by a gamma camera scan (Fig. 19.9). Within a few minutes of injection, the labeled WBC marginates in inflamed bowel and usually increases in intensity over a period of 2–4 h. The WBC scan is a helpful diagnostic tool for the detection of inflammation and abscesses. Soon after it was introduced, the 111In-labeled WBC scan was shown to be highly sensitive in patients with IBD [28]. Subsequently, Technetium TC 99m Hexamethyl propylene amine oxime (99mTc HMPAO) labeled WBC scan was adopted because of ready availability, longer shelf life, lower radiation dose, and superior image resolution [29]. Most pediatric studies indicate that a positive WBC scan is highly predictive of IBD. However, false-negative studies can occur in very early disease or in patients who are in remission due to recent steroid treatment [29–31]. Negative scans have also been observed in children with proximal small bowel disease.

Fig. 19.9
3D volume rendered image from a Tc-HMPAO WBC scan of the abdomen demonstrates intense focal activity in the right lower quadrant (arrow) compatible with the diagnosis of active inflammatory bowel disease of the distal small bowel
Localization of tracer activity can be a useful aid in differentiating children with CD from those with UC. Uptake localized to the small bowel or a more widespread but discontinuous bowel activity correlates highly with CD, whereas in UC the characteristic finding is a continuous pattern of uptake involving the rectum with a variable proximal extension in the colon [29, 32–34]. The WBC scan can also be a reliable indicator of disease activity. A “scan score” calculated by comparing uptake of tracer in affected bowel segments with iliac crest bone marrow activity correlated much better with clinical disease activity than did the erythrocyte sedimentation rate [35]. In the follow-up of patients with known IBD, a negative scan indicates remission and may prompt changes in treatment [29]. The WBC scan may be useful in several areas of clinical decision-making in children with known IBD. A positive WBC scan can identify ileal inflammation when ileoscopy is not feasible [36]. The finding of small bowel activity or skip areas of colonic involvement could help to establish the diagnosis of CD in patients previously assigned the diagnosis of IC [29]. In cases of luminal narrowing, a positive WBC scan may help distinguish active inflammation from fibrosis.
The WBC scan is attractive for children because it is associated with much less radiation exposure than contrast studies. However, scintigraphy has several limitations including false-positive studies in the presence of gastrointestinal bleeding and inability to define anatomic detail including strictures and fistulae [29, 30]. It is also time-consuming, and drawing sufficient blood for labeling can be a challenge in younger children.
Positron Emission Tomography
Positron emission tomography (PET) is a functional imaging technique that has been applied to the detection of inflamed areas of bowel. The high metabolic activity of inflamed tissue results in the uptake of the glucose analog, fluoro-2-deoxy-d-glucose (FDG), which has been radiolabeled with a positron-emitting isotope such as fluorine-18 (F-18). It is transported into cells at a rate proportional to the glycolytic activity of the cell. Within an hour of the intravenous injection of F-18 labeled FDG, the scan is performed, with a total image acquisition time of less than a half hour. PET scanning detects inflamed bowel in children with a reported accuracy similar to the WBC scan [37, 38]. As compared to the WBC scan, PET is faster and does not require blood to be drawn. However, PET scans depend on equipment and expertise that may not be generally accessible. Given the limited availability and the paucity of pediatric studies, PET has a minimal role in the evaluation of pediatric IBD at the present time.
Evaluation of Complications
Perianal Disease
Perianal disease occurs in over one-third of patients with CD but is not associated with UC. Diagnosis of external manifestations, such as skin tags, fissures, ulcerations, and simple perianal abscesses, requires only a careful inspection and digital rectal examination as appropriate. Additional information on complex abscesses, fistulae, and strictures can be obtained by performing an examination under anesthesia (EUA) with procto-sigmoidoscopy and with imaging studies.
Anatomic classification of perianal disease is enhanced by use of modern imaging techniques especially MRI and endoscopic ultrasound (EUS) [39–41]. Anal fistulography has been largely abandoned because of patient discomfort, poor accuracy, and inability to visualize the anal sphincter anatomy [42, 43]. CT is also unreliable in assessing perianal fistulae due to its poor intrinsic contrast resolution that limits its ability to define the anatomy of the levator muscle [44, 45]. Because CT entails exposure to ionizing radiation, it is also disadvantageous in children.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


