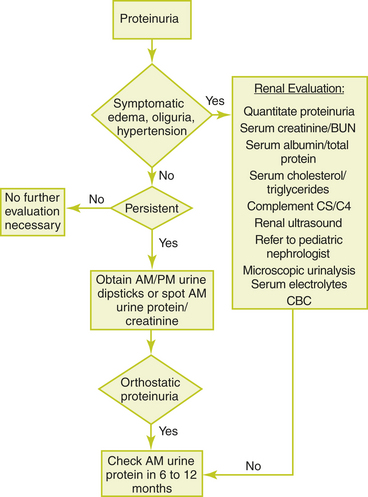
Chapter 36 PROTEINURIA Theodore X. O’Connell General Discussion Most healthy children excrete small amounts of protein in the urine, which is called physiologic proteinuria. Physiologic proteinuria varies with age and the size of the child. When corrected for body surface area, the protein excretion is highest in newborn infants and decreases with age until late adolescence, when adult levels are reached. Asymptomatic or isolated proteinuria is defined as proteinuria not associated with any signs or symptoms of renal disease. The estimated prevalence of isolated asymptomatic proteinuria in children is between 0.6% and 6.3%. However, only 0.1% of children have persistent proteinuria. In general, the finding of proteinuria does not warrant an extensive work-up. The finding of proteinuria must be confirmed on two or three more occasions. Transient proteinuria, the most common cause in children, can be induced by a variety of factors, including fever and exercise. The finding of at least two positive urine tests out of three specimens suggests persistent proteinuria and warrants additional evaluation. Orthostatic proteinuria occurs when urine protein excretion occurs in the upright position but returns to normal when the patient is recumbent. The diagnostic evaluation of the child with dipstick-positive proteinuria is affected by the presence or absence of symptoms. Isolated asymptomatic proteinuria on a urine dipstick, without hematuria, hypertension, or signs of systemic illness or stress, is detected in about 15% of adolescent patients. Only about a fourth of patients have a second dipstick positive for protein if reevaluated within 48 hours, and an even smaller percentage remain positive if tested serially over 6 to 12 months. Therefore, the first step in the evaluation of a child or adolescent with isolated proteinuria is to determine whether the patient has persistent proteinuria in at least two of three urine samples tested 1 or more weeks apart. Once the diagnosis of persistent proteinuria is established, the physician should determine whether the patient has orthostatic (postural) proteinuria. Orthostatic proteinuria accounts for about 60% of children with persistent proteinuria. The patient is instructed to empty the bladder at bedtime, and in the morning a urine sample is immediately collected, which is then tested for protein. Another urine sample is obtained later in the day after ambulation. If the morning urine samples are negative or show trace protein while ambulatory ones are 1+ or greater, a diagnosis of orthostatic proteinuria is made, and no further evaluation is required. However, a urine protein-creatinine ratio should be measured and blood pressure obtained yearly for children diagnosed with orthostatic proteinuria. If the patient has persistent, nonorthostatic proteinuria, a more thorough evaluation is warranted. This includes quantification of proteinuria using either a 24-hour urine collection or a urine protein-creatinine ratio on a spot sample. The urine protein-creatinine ratio has become the preferred method because it is more reliable than 24-hour urinary protein measurements. In adults and children over 2 years of age, a urine protein-creatinine ratio lower than 0.2 on a random urine specimen obtained during the day is considered normal. In children aged 6 to 24 months, the upper limit of normal is 0.5. A ratio above 3.0 is consistent with nephrotic-range proteinuria. The symptomatic child requires more aggressive clinical evaluation. Symptoms may be nonspecific (fever, malaise), more specific but nonurinary (arthritis, rash), or urinary specific (edema, hypertension). The underlying disorder may be renal in origin or secondary to a systemic disease. Children with heavy proteinuria and edema should be evaluated promptly for nephrotic syndrome and, if it is present, have consultation with a pediatric nephrologist. Children with non–nephrotic-range persistent proteinuria who present with hypertension, an abnormal urinalysis, or an elevated plasma creatinine concentration should be evaluated by a pediatric nephrologist. Figure 36-1 provides an algorithm for the evaluation of pediatric proteinuria. Figure 36-1 Evaluation of pediatric proteinuria. (From Mahan JD, Turman MA, Mentser MI. Evaluation of hematuria, proteinuria, and hypertension in adolescents. Pediatr Clin North Am 1997;44:1573–1589.) Causes of Proteinuria Benign persistent proteinuria Orthostatic (postural) proteinuria Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Gynecomastia Abnormal head size and shape Musculoskeletal pain Seizures Stay updated, free articles. Join our Telegram channel Join Tags: Instant Work-ups A Clinical Guide to Pediatrics Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on Proteinuria Full access? Get Clinical Tree
Chapter 36 PROTEINURIA Theodore X. O’Connell General Discussion Most healthy children excrete small amounts of protein in the urine, which is called physiologic proteinuria. Physiologic proteinuria varies with age and the size of the child. When corrected for body surface area, the protein excretion is highest in newborn infants and decreases with age until late adolescence, when adult levels are reached. Asymptomatic or isolated proteinuria is defined as proteinuria not associated with any signs or symptoms of renal disease. The estimated prevalence of isolated asymptomatic proteinuria in children is between 0.6% and 6.3%. However, only 0.1% of children have persistent proteinuria. In general, the finding of proteinuria does not warrant an extensive work-up. The finding of proteinuria must be confirmed on two or three more occasions. Transient proteinuria, the most common cause in children, can be induced by a variety of factors, including fever and exercise. The finding of at least two positive urine tests out of three specimens suggests persistent proteinuria and warrants additional evaluation. Orthostatic proteinuria occurs when urine protein excretion occurs in the upright position but returns to normal when the patient is recumbent. The diagnostic evaluation of the child with dipstick-positive proteinuria is affected by the presence or absence of symptoms. Isolated asymptomatic proteinuria on a urine dipstick, without hematuria, hypertension, or signs of systemic illness or stress, is detected in about 15% of adolescent patients. Only about a fourth of patients have a second dipstick positive for protein if reevaluated within 48 hours, and an even smaller percentage remain positive if tested serially over 6 to 12 months. Therefore, the first step in the evaluation of a child or adolescent with isolated proteinuria is to determine whether the patient has persistent proteinuria in at least two of three urine samples tested 1 or more weeks apart. Once the diagnosis of persistent proteinuria is established, the physician should determine whether the patient has orthostatic (postural) proteinuria. Orthostatic proteinuria accounts for about 60% of children with persistent proteinuria. The patient is instructed to empty the bladder at bedtime, and in the morning a urine sample is immediately collected, which is then tested for protein. Another urine sample is obtained later in the day after ambulation. If the morning urine samples are negative or show trace protein while ambulatory ones are 1+ or greater, a diagnosis of orthostatic proteinuria is made, and no further evaluation is required. However, a urine protein-creatinine ratio should be measured and blood pressure obtained yearly for children diagnosed with orthostatic proteinuria. If the patient has persistent, nonorthostatic proteinuria, a more thorough evaluation is warranted. This includes quantification of proteinuria using either a 24-hour urine collection or a urine protein-creatinine ratio on a spot sample. The urine protein-creatinine ratio has become the preferred method because it is more reliable than 24-hour urinary protein measurements. In adults and children over 2 years of age, a urine protein-creatinine ratio lower than 0.2 on a random urine specimen obtained during the day is considered normal. In children aged 6 to 24 months, the upper limit of normal is 0.5. A ratio above 3.0 is consistent with nephrotic-range proteinuria. The symptomatic child requires more aggressive clinical evaluation. Symptoms may be nonspecific (fever, malaise), more specific but nonurinary (arthritis, rash), or urinary specific (edema, hypertension). The underlying disorder may be renal in origin or secondary to a systemic disease. Children with heavy proteinuria and edema should be evaluated promptly for nephrotic syndrome and, if it is present, have consultation with a pediatric nephrologist. Children with non–nephrotic-range persistent proteinuria who present with hypertension, an abnormal urinalysis, or an elevated plasma creatinine concentration should be evaluated by a pediatric nephrologist. Figure 36-1 provides an algorithm for the evaluation of pediatric proteinuria. Figure 36-1 Evaluation of pediatric proteinuria. (From Mahan JD, Turman MA, Mentser MI. Evaluation of hematuria, proteinuria, and hypertension in adolescents. Pediatr Clin North Am 1997;44:1573–1589.) Causes of Proteinuria Benign persistent proteinuria Orthostatic (postural) proteinuria Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Gynecomastia Abnormal head size and shape Musculoskeletal pain Seizures Stay updated, free articles. Join our Telegram channel Join Tags: Instant Work-ups A Clinical Guide to Pediatrics Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on Proteinuria Full access? Get Clinical Tree