Chapter 2. Problems at birth and resuscitation
Paediatric assistance is requested at around a quarter of all deliveries and some form of support is required in 40% of these cases. Intensive resuscitation, respiratory support at least, is required at 3% of all deliveries. This chapter will cover the commoner problems that may lead to difficulties at delivery and in the early postnatal period and will emphasise the standard approach to resuscitation that is taught on the Resuscitation Council Neonatal Life Support Course. 1 With the current quality of antenatal imaging many problems can be detected in pregnancy (60–80% of major and 35% of minor abnormalities by routine screening at 18–20 weeks) and an appropriate early management plan can be initiated. However, unexpected problems will always occur and it is thus essential that all staff have the skills necessary to deal with these situations.
| Neonatal Life Support Algorithm |
| Dry and wrap |
| ↓ |
| Assess – breathing, heart rate, colour, tone |
| ↓ |
| Open airway |
| ↓ |
| Re-assess |
| ↓ |
| Inflation breaths – 5 breaths; 2–3 seconds; 30cmH 2O |
| ↓ |
| Re-assess |
| ↓ |
| Ventilation breaths – for 30 seconds: 30/minute; 25cmH 2O |
| ↓ |
| Re-assess |
| ↓ |
| Cardiac compressions – (assuming good chest movements and no improvement in heart rate) 3 compressions to one breath |
| ↓ |
| Re-assess after 30 seconds |
| ↓ |
| Drugs |
| If the chest fails to move |
| Check head position |
| ↓ |
| Single person jaw thrust |
| ↓ |
| Two person jaw thrust |
| ↓ |
| Clear airway under direct vision |
| ↓ |
| Guedel airway |
QUESTION 1
You are called to a delivery of a term baby where profound decelerations have been seen on the CTG. The baby is born in poor condition and there is thick meconium in the liquor and on the baby’s skin.
i) Which of the following manoeuvres are appropriate? Give one answer.
a. Perineal suction
b. Clamping the chest
c. Tracheal lavage with normal saline
d. Immediate intubation and tracheal suction
e. Dry and wrap.
The baby is not breathing and is white and hypotonic with a heart rate is 30 bpm. Initial T-piece ventilation fails to obtain chest movement.
ii) What two forms of immediate treatment are appropriate?
a. Start cardiac compressions immediately
b. Repeat inflation breaths
c. Continue with ventilation breaths
d. Prepare for drug administration through the umbilical vein
e. Immediate intubation
f. Check head position
g. Visualise the oro-pharynx.
Following tracheal suction, chest movement is obtained. After 30 seconds of ventilation, the heart rate remains at 30 bpm.
iii) What two immediate actions are indicated?
The baby is transferred to the neonatal unit and requires ventilation. Initial ventilatory settings are:
Pressures 30/4, FiO 2 1.0, rate 40, Ti 0.4 s, flow 4 L/min
His initial arterial gas is as follows:
| pH | 7.03 |
| PCO 2 | 10.6 kPa |
| PO 2 | 4.5 kPa |
| BE | –10.6 mmol/L |
| Bicarbonate | 17.5 mEq/L |
v) What ventilation manoeuvres could you do to improve the gas?
a. Increase PIP
b. Increase Ti
c. Increase PEEP
d. Increase oxygen
e. Decrease Te
f. Increase flow
g. Decrease flow.
vi) What additional treatments could be considered?
At 2 hours of age, the baby develops a tension pneumothorax. Following drain insertion, the following chest X-ray is obtained.
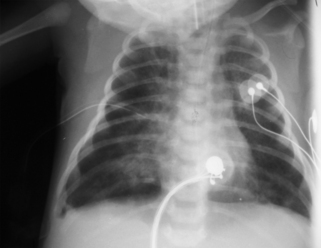 |
| Figure 2.1. |
vii) List five abnormalities on the chest x-ray.
At 6 hours the following gas is obtained:
| pH | 7.18 |
| pO 2 | 2.8 kPa |
| pCO 2 | 8.3 kPa |
| BE | –9.6 mmol/L |
| Bicarbonate | 22.1 mEq/L |
Ventilatory settings are:
Pressures 35/5 cmH 20, MAP 17, FiO2 1.0, Ti 0.4 s, rate 60
viii) What is the oxygenation index?
ix) What is the most likely diagnosis?
x) List four possible treatments.
QUESTION 2
You are asked to review a baby on the postnatal wards 12 hours of age after a difficult delivery. The baby is said to be fractious and is not feeding. As part of a septic screen, a chest x-ray is carried out.
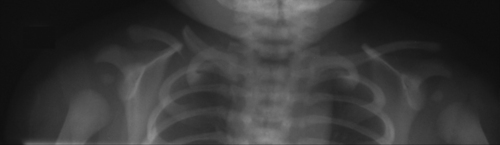 |
| Figure 2.2. |
What abnormality does this x-ray show?
QUESTION 3
On a first day check, a baby is noted to have an absent red reflex.
i) What is the most likely diagnosis?
a. Retinoblastoma
b. Cataract
c. Glaucoma
d. African race.
ii) What is the most important action and why?
QUESTION 4
You are called urgently to the postnatal wards to see a baby. He was born at term by normal vaginal delivery with good Apgars and was feeding well for the first 2 days. Since this morning his mother has noticed that he is floppy, and not interested in feeds. The midwife has just been called to see him as his mother has tried to wake him for a feed and cannot rouse him. He is pale with cold peripheries, capillary refill time is 7 seconds, respiration is shallow, pulses are weak and heart rate is 180 bpm.
i) What are the two most likely diagnoses?
a. Intracranial haemorrhage
b. Sepsis
c. Inborn error of metabolism
d. Hypoglycaemia
e. Hypernatraemia
f. Hypocalcaemia
g. Duct-dependent congenital heart disease
h. Hypoxic–ischaemic encephalopathy.
ii) What two immediate actions would you undertake?
iii) What three investigations would be most useful in directing early management?
iv) What three investigations would be most helpful in establishing the differential diagnosis?
vi) The following blood count is obtained:
| Haemoglobin | 18.6 g/dL |
| WBC | 25×10 9/L |
| Neutrophils | 15×10 9/L |
| Lymphocytes | 8.5×10 9/L |
| Monocytes | 1.1×10 9/L |
| Eosinophils | 0.4×10 9/L |
| Platelets | 155×10 9/L |
With this information what is the most likely diagnosis?
vii) While waiting for an echocardiogram you obtain the chest x-ray shown below.
 |
| Figure 2.3. |
Describe the abnormalities.
viii) With this information what is your diagnosis and action?
ix) Parents are anxiously waiting for further information. What are you going to tell them?
QUESTION 5
i) Give three indications for postnatal administration of BCG.
ii) Give three contraindications for postnatal administration of BCG.
QUESTION 6
A baby is born following a ventouse delivery. Mother has noticed a swelling on the side of the head. Choose four features that would allow you to discriminate between a caput, cephalhaematoma and a subgaleal haematoma (subaponeurotic haematoma).
a. Location
b. Demarcation
c. Jaundice
d. Clinical time course
e. Petechiae
f. Bruising
g. Erythema
h. Time of presentation
i. History of instrumental delivery
j. Coagulation
k. Blood count.
QUESTION 7
You are asked to see a baby who has the obvious features of a brachial plexus injury.
i) How do you differentiate between an Erb and a Klumpke palsy?
ii) The parents want to know why it happened, how common it is, what treatments are available and what the long-term outcome is likely to be.
QUESTION 8
A baby has been born by difficult instrumental delivery. You are asked to review the baby and skull imaging is performed. The following picture is obtained.
 |
| Figure 2.4. |
i) What does the X-ray show?
ii) What management is indicated and why?
QUESTION 9
A baby is born by normal vaginal delivery. A right sided facial palsy is noted and the right eye cannot be fully closed.
i) What is the most likely cause, and what immediate action would you consider?
ii) Which of the following syndromes are associated with a facial palsy? Choose three.
a. Cardiofacial syndrome
b. Edwards syndrome
c. CHARGE syndrome
d. Möbius syndrome
e. Poland sequence
f. Goldenhaar syndrome.
iii) The palsy persists and appears unchanged at an outpatient appointment two weeks later. What course of action would you recommend?
On more detailed examination in clinic, the infant is noted to have an inability to abduct the left eye. In addition there is mild talipes equinovarus and what appears to be a lack of chest wall bulk on the right side. There is also mild micrognathia and microtia.
iv) What syndrome is most likely?
v) What medication used in pregnancy is associated with this syndrome?
vi) What is the most likely long-term outcome if this diagnosis is correct?
QUESTION 10
A term baby presents with an intracranial bleed and gastrointestinal bleeding. He has not had vitamin K prophylaxis. Which of the following coagulation results will confirm the diagnosis of vitamin K deficiency bleeding? Choose three.
i) Normal PT, Normal APPT, Normal Fibrinogen, Normal Platelets
ii) Prolonged PT, Normal APPT, Normal Fibrinogen, Normal Platelets
iii) Prolonged PT, Prolonged APPT, Low Fibrinogen, Low Platelets
iv) Normal PT, Normal APPT, Normal Fibrinogen, Low Platelets
v) Very prolonged PT, Moderately prolonged APPT, Normal Fibrinogen, Increased Platelets
vi) Very prolonged PT, Moderately prolonged APPT, Increased Fibrinogen, Normal Platelets
vii) Normal PT, Prolonged APPT, Decreased Fibrinogen, Normal Platelets
QUESTION 11
A 37 week gestation infant is admitted following an elective caesarean section. She has become tachypnoeic and a radial artery line has been inserted. She is noted to have a bruise on her left leg and a clotting screen is sent. The following result is obtained:
| PT | 17 seconds |
| APPT | 84 seconds |
| Fibrinogen | 2.5 g/L |
| Platelets | 449×10 9/L |
i) What does this coagulation result show?
ii) What abnormal conditions may explain it?
iii) What other explanation is possible?
iv) How would you distinguish between the possible causes?
QUESTION 12
A woman is admitted on to delivery suite at term. The CTG is abnormal with marked decelerations to 40 and a baseline bradycardia. She is taken immediately to theatre for an emergency caesarean section, and the baby is born 15 minutes later. At delivery the baby is white, floppy, and the heart rate is very slow.
i) What are your first actions? List four.
There is no respiratory effort, the heart rate is 20 bpm, and the baby is white and floppy.
ii) What are your next four steps?
The chest is seen to move well; however the heart rate remains at <20 bpm, and the baby is still white and floppy.
iii) What are your next actions? Suggest three.
The baseline heart rate remains at around 20 bpm. Good chest movement continues. You insert an umbilical venous catheter.
iv) What is the first thing you will do after successful placement?
v) Heart rate remains slow. You decide to give resuscitation drugs.
a. What will you use?
b. How much will you give?
c. What order will you give them in and what is your rationale for doing so?
With the drugs you have administered, the heart rate rises to approximately 60 bpm but no further. Ventilation remains effective. The blood tests you send from umbilical venous blood are reported back as:
The heart rate rises a little further to 75 bpm. The baby remains very white and floppy. Further blood results come back with a haemoglobin from the umbilical venous sample of 15.2 g/dL. However, the obstetrician performing the C/S reports that there was ‘an awful lot of blood about’.
vii)
a. What else might you consider?
b. What action would you take?
Following this action, the heart rate rises to >100 bpm but there is still no respiratory effort. The baby remains floppy and does not respond to stimulation. You admit the baby to the neonatal intensive care unit, and initiate positive pressure ventilation at pressures of 20/4, I:E ratio 0.3:0.8 seconds, FiO 2 0.21.
viii) What baseline monitoring would you consider? List six.
ix) What baseline investigations would you perform? List five.
Half an hour after admission, the following results are obtained from an arterial line:
pH 7.3, pCO 2 3.1 kPa, BE –15.5 mmol/L, lactate 9 mmol/L, Hb 10.2 g/dL
x) What three actions would you consider?
The nursing staff report oxygen desaturations on the monitor. They are uncertain as to whether there are associated abnormal movements. The baby remains extremely floppy.
xi) What further baseline investigations would you perform? Name six.
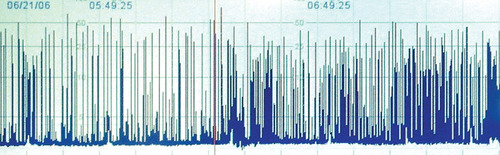
CFAM is commenced and the following trace is obtained.
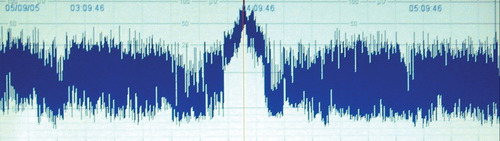 |
| Figure 2.5. |
xii)
a. Describe the trace. Is it normal?
b. What key features have led to your conclusion?
xiii) What treatment modalities would you consider?
xiv)
a. What is your first line medication for this condition?
b. What dose would you prescribe (the baby weighs approximately 3.5 kg)?
Despite this treatment, there is no improvement in the baby’s condition. The CFAM at this point is shown below.
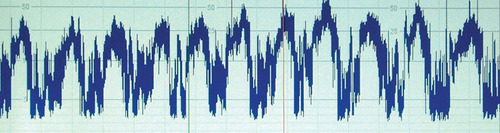 |
| Figure 2.6. |
xv) Describe the trace.
xvi) What do you do now?
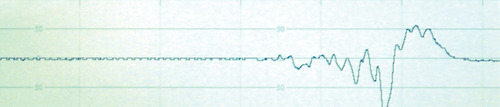
xvii) Following this treatment, the baby’s clinical condition seems to stabilise, but the CFAM at this point is below.
 |
| Figure 2.7. |
Describe the trace.
xviii) What other complications may this baby sustain and how would you assess them?
As part as a more detailed assessment, cranial ultrasonography is performed with Doppler studies of the anterior cerebral artery. The cerebral blood flow velocity is more than 3 SD from the mean and the PRI (Pourcelot Resistance Index) is 0.5.
xix) Explain the significance of these observations.
At 24 hours of age, the baby is anuric, urea 9.2 mmol/L, creatinine 165 μmol/L. Blood pressure is persistently low with a mean BP of 28–30 mmHg despite inotropic support. Echocardiography shows very poor myocardial contractility. Assessment of liver function shows markedly elevated transaminases and gamma-GT. The baby is profoundly hypotonic and unresponsive to painful stimuli. A formal EEG is performed and the following trace obtained.
 |
| Figure 2.8. |
xx) What does this show?
xxi) What would be the main areas of discussion that you would have with the parents?
QUESTION 13
You are informed of the imminent delivery of a baby at 25 weeks gestation.
i) In the few minutes you have before delivery what specific areas of preparation will you concentrate on? List five.
ii) The infant is delivered and cries at birth. What immediate measure can be taken to minimise heat loss?
iii) What actions should you take to optimise ventilatory support immediately after birth?
QUESTION 14
You are called to see a baby boy on the postnatal wards who has had difficulty feeding. On examination the baby is noted to be floppy and has normal tendon reflexes. There are spontaneous anti-gravity movements. There is no fasciculation.
i) Is this central or peripheral hypotonia?
ii) What could be the likely cause? Choose two.
a. Spinal muscular atrophy
b. Prader–Willi syndrome
c. Hypothyroid
d. Congenital myotonic dystrophy
e. Congenital myasthenia.
On further examination the baby is noted to have undescended testes and almond shape eyes.
iii) What is the most likely diagnosis?
iv) What test would confirm your diagnosis?
v) Which of the following endocrine problems is recognised as a characteristic finding in Prader–Willi Syndrome?
a. Hypothyroidism
b. Hypoinsulism
c. Hypoparathyroidism
d. Hypopituitarism
e. Hypoaldosteronism.
ANSWER 1
i)




e. Dry and wrap.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
