44 Primary and Acquired Immunodeficiency Disorders
The initial eight cases of pediatric acquired immunodeficiency syndrome (AIDS) were reported in 1983 from the Pediatric Allergy-Immunology and Infectious Disease program in Newark, New Jersey, initially named the Children’s Hospital AIDS Program (CHAP).1 When the children’s hospital closed in 1998, the Pediatric HIV/AIDS program was renamed the François-Xavier Bagnoud Children Center. One of the cases from this initial cohort best illustrates the recognition that these infants and children were part of the AIDS epidemic and not a sudden increase in a new form of primary severe combined immunodeficiency disorder (SCID).
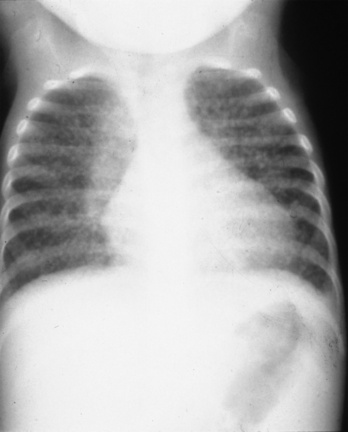
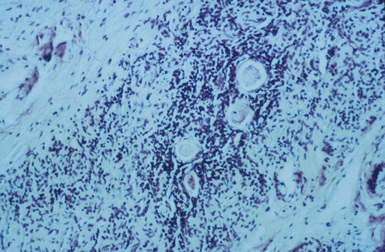
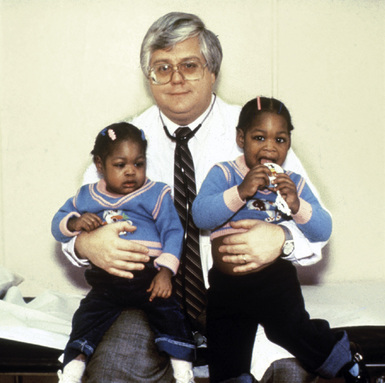
A 4-month-old girl presented with chronic diarrhea, leading to failure to thrive and wasting syndrome that was associated with recurrent and severe sino-pulmonary infections anemia, lymphopenia, generalized lymphadenopathy and thrombocytopenia. She was under the supervision of New Jersey’s Division of Youth and Family Service (DYFS) by a foster mother, because of abandonment by her chronically ill intravenous drug-using mother. Her initial immunologic laboratory evaluation showed a surprising hypergammaglobulinemia instead of the expected hypogammaglobulinemia, low total T cells and, as was typical for that era, low markers by immunoflorescent microscopy for helper T cells. A lung biopsy was done for chronic infiltrates. During the procedure there was little thymus tissue noted and a small piece was obtained for pathologic evaluation. The lung biopsy demonstrated severe lymphocytic iterstitial pneumonia (LIP) (Fig. 44-1) and the thymus biopsy was reported as showing chronic inflammation, calcified Hassall bodies with marked reduction in thymus lymphocytes. These changes were unexpected and consistent with a probable chronic perinatal infection (Fig. 44-2). Most importantly, she had an identical second-born twin sister who was and remains healthy (Fig. 44-3). Over time, HIV/AIDS was confirmed in the ill twin while her identical twin sister remained well and thriving with consistently negative HIV assays. Both are now 30 years old and the HIV-infected sibling has survived despite progression of her HIV to AIDS. Until specific HIV diagnostic studies became available, the care team, including one of the coauthors of this chapter (JO), diagnosed differentiated perinatal HIV from the assumed initial diagnosis of SCID, based on the unexpected results of lung and thymus tissue and the discordant clinical course of the twins.
Epidemiology of Inherited and Acquired Immunodeficiency Syndromes in Childhood
Approximately 55,000 children, newborn to age 19, die in the United States annually, with nearly half of these deaths being infants, of which two thirds are neonates.2 These infant mortalities are mostly due to prematurity as well as congenital and/or genetic abnormalities, both having primary or secondary immune dysfunction. Most of these secondary immune problems in the premature infant are related to innate immune dysfunction that include breaks in skin and mucus membrane integrity, nutritional deficiencies, exposure to nosocomial infectious agents and exposure to frequent procedures and broad-spectrum antibiotics. In older children, worldwide mortality has been decreasing, with most deaths attributed to chronic, life-limiting medical conditions. Primary and secondary immunodeficiencies in infants contribute considerably to infant mortality and pose a significant, but often not recognized, threat to the health and well-being of children in the United States.
Primary or inherited immunodeficiencies are almost always genetically determined, often confined to a few rare, familial, monogenic, recessive traits that impair the development or function of one or several leukocyte subsets and result in multiple, recurrent, opportunistic infections during infancy. With improved diagnostic capabilities and an increased understanding of human immune functions, these immunodeficiencies are proving to be more common than previously estimated and may affect a much larger population because of a broadening of the definition of primary immunodeficiencies (PID). Considerable expansion of the understanding of immunological changes is being demonstrated in multiple chronic diseases, as well as improved survival with more effective treatments (Table 44-1).3 The frequency of PID varies in different countries, with certain populations having higher frequency of some specific PID mutations.4 Progress in medical care has made it possible for many of these children with PID to survive to adulthood with symptoms and complications that may not be recognized by adult primary care providers.5
TABLE 44-1, A Classification of Primary Immune Disorders That Manifest in Neonates
| Components of the immune disorder | Immune system | Inheritance / associated features |
|---|---|---|
| Predominant antibody defects | ||
| Predominant defects in cell-mediated immunity | De novo defect or AD/conotruncal malformation; hypoparathyroidism: cardiac outflow tract malformation; abnormal faces/common | |
| Combined antibody and cellular immunodeficiencies | Wiskott-Aldrich Syndrome | XL/thrombocytopenia; small defective platelets, eczema; lymphoreticular malignancies; autoimmune disease |
| Severe combined immunodeficiencies | XL/symptoms may be similar to GVH disease in neonatal period (maculopapular rash, alopecia, lymphadenopthy)/rare | |
| Defects of phagocytic function | ||
| Complement deficiencies | C5, C6, C7, C8a, C8b, C9 deficiency | AR/neisserial infections, SLE/very rare or rare |
| Auto Inflammatory disorders | Neonatal onset multisystem inflammatory disease (NOMID) or chronic infantile neurologic cutaneous and articular syndrome (CINCA) | AD/Neonatal onset rash, chronic meningitis, and arthropathy with fever and inflammation in response to IL-1R antagonist (Anakinra)/very rare |
Notarangelo L et al. International Union of Immunological Societies Expert Committee on Primary Immunodeficiencies: Primary immunodeficiencies: 2009 update. J Allergy Clin Immunol 2009: 124:1162 –1178.
Secondary or acquired immunodeficiencies are more common than primary disorders of immune function (Table 44-1, B). By far, the most common secondary immunodeficiency of this era is HIV/AIDS.6 Based on the original version of the PACTG 219 follow-up study from 1993 through 2000, Table 44-2 lists the most common diagnosis during that period when HAART therapy was not available.7 Unfortunately, children presenting with these diagnoses at birth through 4 years also experienced the highest mortality rate. In the older age groups, Pneumocystis jirovecii pneumonia (PCP) remained associated with a high mortality rate but lymphocytic interstitial pneumonia (LIP) was a marker for prolonged survival before HAART therapy.8 Sadly, during the early epidemic, despite a high morbidity and mortality rate, most attention was focused on treatment of opportunistic infections with little attention given to palliative and supportive care.
TABLE 44-1, B Classification of Immune Disorders Associated with or Secondary to Other Diseases
| Disease | Immune disorder | Inheritance / associated features |
|---|---|---|
| Bloom syndrome | Reduced T-cell function and decreased IgM | AR/LBW, retarded growth, facial telangiectasia, sun-sensitive erythemia, increased susceptibility to malignancies, molar hypoplasia, bird-like face/ rare |
| Fanconi anemia | Decreased T lymphocyte and natural killer (NK) cell function, decreased IgA | AR/multiorgan defects, bone marrow failure, café au lait spots, limb defects, abnormal faces, hyperpigmentation |
| Xeroderma pigmentosa (XP with 7 subgroups A-G and a variant, XPV) | Decrease in CD4+ levels and function due to mutation of the DNA repair gene for ultraviolet (UV) induced damage. | AR/defect in nucleotide excision repair (NER) with mutations of important tumor suppressor genes (e.g., p53 or proto oncogenes) leading to a sixfold increase in metastatic malignant melanoma and squamous cell carcinoma as well as XP being six times more common in Japanese people |
| Cancers | Bone narrow suppression from tumor infiltration or ablation of marrow from therapy: drugs or radiation | An increasing number of cancers appear to be enhanced by specific genetic characteristics |
| Malnutrition | Both single nutrient/trace metal impact on specific immune function or generalized wasting | AR/acrodermatitis enteropathica (zinc deficiency) |
| Infections | Varies with organism and whether localized/systemic or acute/chronic | Chronic, multiorgan system viral infections predominate, penultimate example being HIV/AIDS |
| Prematurity | Greatest impact on innate host defenses | More profound when gestation <28 weeks because of sharp drop in maternal-to-fetus transfer of immunoglobulins |
| Chronic organ system diseases: diabetes or renal disease | Like infections, great variations with severity depending on single or multiple organ involvement, timing of onset | Depending on organ systems or specific cause of organ failure, there may be a genetic-linked immuno deficiency syndrome |

Globally, an estimated 430,000 children younger than 15 were newly infected with HIV in 2008. The vast majority of these children (90%) acquired the virus via perinatal/mother-to-child transmission (MTCT). By the end of 2008, 2 million children were infected with HIV worldwide, with 280,000 children dying of the disease in that same year.9 In the United States, HIV has become the sixth-leading cause of death among 15-24 year-olds,10 and continues to disproportionately affect people of color. African Americans, who account for only 13% of the U.S. population, represent 51% of the estimated number of HIV/AIDS diagnoses made through 2007.11
HIV is also transmitted via other routes, such as through blood transfusions as evidenced in the hemophilia population. Before the policies for screening HIV in blood supplies were instituted, many people were exposed to the virus through intravenous transfusions of blood or blood products. People with hemophilia routinely need certain blood-clotting components, and receive them through frequent blood transfusions. From 1978 through 1985, many hemophiliacs were inadvertently put at extremely high risk for acquiring HIV through the public blood supply. Hemophiliacs now represent 1% of all people with AIDS in the United States.12
The final group of children who acquire HIV are victims of sexual abuse. A small percentage of children (<1%) acquire HIV through sexual abuse by an infected adult male, usually a relative or close friend of the family. Because sexual abuse of children is likely to be under-recognized and under-reported, sexually abused children are not routinely screened for HIV infection, and sexually abused children infected with HIV who have not progressed to AIDS are not reported in many states, the full extent of sexual transmission of HIV among children is not known.13 It is important to also note that among adolescents ages 15 to 19, the major cause of HIV infection is through high-risk sexual activity.



