56 PREOPERATIVE EVALUATION (NONCARDIAC SURGERY)
General Discussion
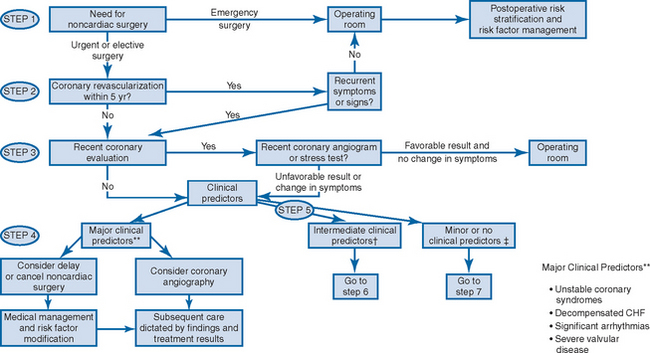
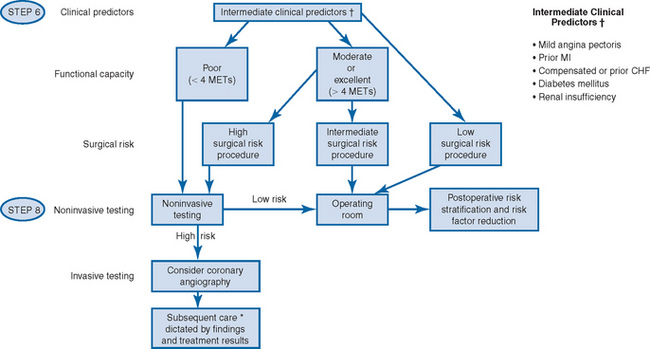
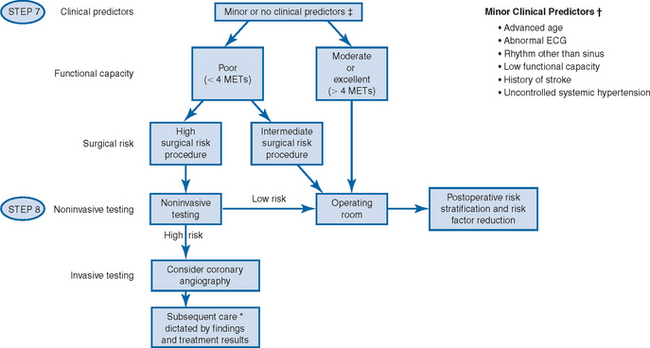
Recommendations do not call for preoperative cardiac testing in all patients. The need for cardiac evaluation is determined by the clinical risk factors identified from the patient’s history, physical examination, functional status, EKG, and the risks inherent to the procedure being considered. Figure 56.1 provides the guidelines of the American College of Cardiology and the American Heart Association.
The role for preoperative pulmonary function testing remains controversial. The American College of Physicians recommends spirometry in patients with a history of dyspnea and tobacco use who are undergoing upper abdominal or coronary artery bypass surgery. For any patient with cough or dyspnea, a work-up should be performed to evaluate for the underlying etiology. Asthma should be under control before surgery if possible. Any pulmonary infection should be treated preoperatively.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


