37 Prenatal and Neonatal Palliative Care
For most, pregnancy is a time filled with joyful anticipation of welcoming a new life into the family. Technological advances provide early confirmation of pregnancy, thus allowing parents to share their news with others, often just weeks after conception. Technology also permits clinicians to detect life-threatening fetal complications. Each year in the United States, more than one million pregnancies will end in fetal death, many due to genetic abnormalities. More than 26,000 babies between 20 and 40 weeks’ gestation will be stillborn, and nearly 18,000 neonates will die within the first 28 days of life, with nearly half of these deaths due to congenital diseases and/or prematurity.1 Gestational risk factors such as a family history of genetic diseases or maternal chronic illness can result in repeated losses.
Families may learn that their baby has a life-threatening fetal diagnosis early in pregnancy, in the prenatal period just prior to delivery, or in the neonatal period after birth. As parents learn of a life-threatening fetal condition, they bear the difficult task of shifting from joyful welcoming of new life to comprehending the ramifications of their baby’s diagnosis. Palliative care in each scenario is targeted to families’ unique needs after diagnosis, when families begin to grieve the loss of a “normal” pregnancy or infant.2 Fetal-neonatal conditions that would benefit from the interventions and support of palliative care can include rare syndromes such as anencephaly and Potter’s syndrome, all extremely premature infants, and infants with severe birth injuries. We will describe how interdisciplinary clinicians can deliver integrated, compassionate, and evidence-based services for these infants and families.
In this chapter, we discuss prenatal-neonatal palliative and end-of-life care. Often the term perinatal is used to describe care around the time of birth; we will use prenatal and neonatal to be more precise. We will highlight the unique contributions of interdisciplinary team (IDT) clinicians, as related to four distinct periods (Fig. 37-1):

IDT Clinicians and Roles
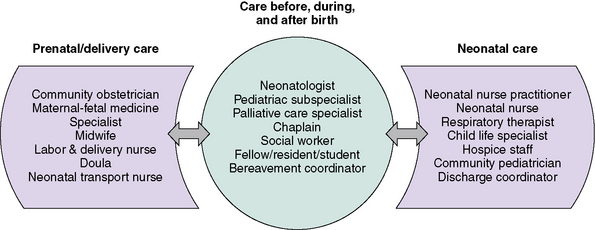
The diagnosis and management of a life-threatening condition for an infant can span the prenatal and neonatal periods, and may require the involvement of unique interdisciplinary team clinicians not found in other areas of pediatric palliative care (Fig. 37-2). Not uncommonly, IDT clinicians work in different clinics, hospitals, or even cities due to the nature of regionalized neonatal care. For example, a life-threatening fetal diagnosis may be made by a community obstetrician, with subsequent management of both mother and baby by multiple subspecialists at a large referral center. Particular effort must be made to communicate well and to provide seamless care to families throughout this trajectory of care.
Supporting families’ practical needs
Mothers with a high-risk pregnancy are often hospitalized for a prolonged period before birth. The mother’s hospitalization can profoundly disrupt the life of the family, and mothers often worry about this burden on their loved ones.3 Distance from home to the regional hospital may be significant, with the associated costs of travelling and parking. Families with a limited income may be forced to visit during late hours when parking is free, which can affect communication with daytime care providers.
Environments that are conducive to and promote family presence are essential. Privacy and lenient visitation hours are important to women hospitalized prenatally.3 When private rooms are not available, strategies are needed to maintain confidentiality during parent-provider discussions. Parents are very cognizant of and appreciative for those clinicians who go out of their way to enable family members to be present with them at their time of distress.4
Siblings may be aware of a baby’s expected arrival before the life-threatening fetal diagnosis is made. Siblings have their own feelings of anticipation, excitement, sadness, or ambivalence. IDT clinicians may need to provide families with strategies to allow siblings to maintain closeness with their mother during her hospitalization while maintaining as normal of a home routine as possible. Parents may need suggestions about how to include their children in the events surrounding the baby’s birth and death.5 Child life specialists can offer creative avenues of art, play, and interactive therapies to assist these children as they meet and say good-bye to their baby brother or sister.
Communication
The importance of clear, honest, and compassionate communication is central to prenatal and neonatal palliative care.6–9 Clinicians can convey empathy through careful listening and anticipation of the family’s needs. Respect is apparent when clinicians refer to the baby by his or her given name. Respect extends to colleagues when conflicting opinions, which often arise in prenatal and neonatal decision- making, are approached in a professional manner. A family’s confidence and trust in the healthcare team are eroded if they witness disrespectful behavior among members of the team. An example of disrespectful behavior is when clinicians are openly critical of the competency of their colleagues because of a disagreement with a medical diagnosis and/or a management decision. These conversations should never occur in the family’s presence or where the conversations could be overheard. A family needs to know that clinicians work collaboratively as a team and with the family to identify a plan of care.
Decision-making
Internationally, there is significant variation in the process of decision-making for these infants. In countries with paternalistic models of medical care, physicians decide which infants will receive life-sustaining therapies, without family input.10 In the United States, parent-provider collaboration in shared decision-making has become increasingly important. Neonatologists acknowledge that, at times, family autonomy in decision-making may even surpass the authority of the medical team.11–13 For instance, a neonatologist may not feel comfortable limiting delivery room resuscitation for an infant born at  weeks’ gestation if the family requests that “everything be done,” even when the likelihood of survival is extremely low.
weeks’ gestation if the family requests that “everything be done,” even when the likelihood of survival is extremely low.
Best practices for engaging in shared decision-making before, during, and after birth are not clear. Ideally, multiple interdisciplinary discussions would occur with families over time while minimizing the stressors of maternal illness, pain, and disruption of the family’s home life. But this rarely occurs. While data about these interactions are limited, retrospective data suggest that parent-provider collaboration in these scenarios is incomplete. A study interviewing the parents and neonatologists within 24 hours of counseling showed there was only 59% agreement that a management plan had been formulated.14
Parents and providers may come to these conversations with very different priorities. Neonatologists often emphasize predictions of morbidities and mortality,15–17 yet families often focus on emotions, hope, and religious and spiritual beliefs.18,19 Those who became pregnant through assisted reproduction or who have suffered repeated losses may be particularly committed to continuing a pregnancy, regardless of predictions of illness or death.20 Families may possess unrealistic expectations for their infant based on media portrayal of “miracle babies.”
As with older children, parents have the right to act as surrogate decision makers for their infants. But surrogate decision-making for infants is unique in several ways. The concept of prior preferences does not apply to newborns. Parents and providers may differ significantly in their perceptions of a “good” quality of life for infants; in one study, parents were more likely than providers to believe that attempts should be made to save all infants, regardless of projected outcomes.21 New parents already expecting to bring home a totally dependent infant may underestimate the consequences of decisions that may extend this dependence indefinitely.
Families must be cautioned that, once a decision is made, diagnostic and prognostic uncertainty may translate into unexpected outcomes. The family who makes a carefully detailed birth plan involving out-of-state family members and religious rituals may suffer a fetal death before birth. Families who opt for non-resuscitation of an extremely premature infant to prevent infant suffering may deliver a vigorous baby weighing 200 g more than predicted. Providers and families alike should prepare for the possibility that management decisions may need to be altered quickly based on new information.22–24
Finally, it should be noted that not all management options are equally available to families. Hospital and state policies can impact provider willingness to offer the options of pregnancy termination, non-initiation of resuscitation, and withdrawal of therapy.25,26
Hope
Redefining hope is critical during prenatal and neonatal palliative care. Families are often unprepared for the diagnosis of a potentially lethal fetal or neonatal condition. Physicians may worry that talking about hope will create unrealistic expectations, yet parents who have gone through this have emphasized that, regardless of the infant’s prognosis, parents need providers to give them hope for something.18,19,27 One study found that physicians who provided more hope to families were not necessarily more likely to predict survival, but they did express emotion and showed parents that they were touched by the tragedy of the situation.18 Adult patients with a terminal diagnosis said providers can provide hope by shifting the focus to what can be realistically achieved versus what can only be wished for.28 For the IDT that is counseling a family, this might mean openly acknowledging the grief and pain of the situation, reassuring the family that the team will join in their hope that the infant’s outcome will be a good one, and helping them to imagine how they might want events to proceed if the outcome is death or severe disability.
It is helpful to talk with families about what is meaningful to them, such as the possibility of holding a baby who is alive, or making sure that the infant does not experience pain. Hope for a good outcome may need to be redefined repeatedly over time in a way that helps families to cherish what is possible with their infant. For parents expecting multiple babies, parental hope for each of the developing fetuses in utero may hang in a delicate balance, especially if one is diagnosed with a life-threatening condition. When the death of a multiple occurs, parents must simultaneous maintain hope for the surviving babies while experiencing grief for their loss.29
Cultural, religious, and spiritual issues
Families often struggle to make meaning of a child’s death in the context of their cultural, religious, spiritual, or existential beliefs. This struggle may inform the decisions families make regarding their infant. A 2010 text30 provides an excellent reference for neonatal end-of-life care issues as related to a number of religious traditions. Several aspects of religion and prenatal and/or neonatal end-of-life care should be noted. In some traditions, a fetus is not recognized as a person until it is born alive. Parents from these traditions who experience a miscarriage or stillbirth may feel abandoned by their communities, and may need additional resources from the IDT. In other traditions, families may struggle to reconcile pregnancy termination or withdrawal of neonatal care with religious doctrine. Talking with their own religious leader and/or a hospital chaplain can be invaluable, both by alleviating family guilt and by helping the medical team to better understand the parents’ values. Obstetric and neonatal wards often limit visitors; accommodations need to be made for families’ cultural or religious end-of-life rituals. One advantage of home hospice for infants is the opportunity for families to more freely participate in religious and cultural rituals.
Professional Caregiver Suffering and Moral Distress
As in other areas of pediatric palliative care, being with families throughout their baby’s dying can be deeply rewarding but can also lead to suffering by the professional caregiver. Suffering is intensified in situations involving moral distress, which often characterizes the uncertainty of prenatal and neonatal prognosis.31 Tragic infant deaths and cumulative losses can make it difficult for a clinician to create meaning in his or her profession. clinicians who themselves are childbearing or childrearing may closely identify with families, particularly when clinicians have a long-term relationship with the family. Though such sensitivity can promote empathy in the clinician, it can also cause death anxiety and grief. A dual-process model of clinician’s grief has been described: clinicians will simultaneously experience grief reactions by focusing on the loss and avoiding grief reactions by focusing on other aspects of a patient’s care.32,33
Infant deaths often occur in environments that do not support clinicians’ needs. Prenatal deaths may occur in birth centers, where care is focused on healthy births, often evidenced by names such as the New Life Center. Clinicians in birth centers may struggle to care for bereaved families while simultaneously caring for parents who are birthing healthy infants.34 Neonatal deaths often occur in intensive care units, which rarely emphasize the sacredness of the end-of-life experience. Though clinicians may join in annual rituals to honor deceased patients and their own grief, support during acute losses may not be available.
IDT clinicians from varying disciplines have unique experiences with families at the end of life. For example, while neonatal nurses rarely feel involved in decision-making, neonatal physicians feel very responsible for end-of-life decision-making.35 These differences may make it difficult for providers to fully support each other. IDT clinicians, such as chaplains, with expertise in addressing suffering could facilitate self-care for others.
Strategies for minimizing professional caregiver suffering must also take place at the organizational level. An educational intervention in end-of-life care, which included content on prevention of compassion fatigue, has been shown to increase the comfort of neonatal nurses who care for a dying infant.36 Other strategies might include a core group of clinicians to serve as a resource on all shifts, case reviews of each death for all disciplines, engaging mental health liaisons for debriefing, and providing meaningful gestures to clinicians, such as massages. Co-creation of ritual may provide clinicians with opportunities to both support bereaved families and facilitate their own grief work33 (Fig. 37-3).

The Four Periods of Prenatal and Neonatal Palliative Care
Early prenatal palliative care
Setting
As illustrated in the case study, EPP palliative care may begin in the obstetrician’s office. Further evaluation may involve specialist consultations at a regional hospital far from the family’s home. In some instances, diagnosis of a specific prenatal condition, such as twin-to-twin transfusion or monoamniotic twins, may require the parents to travel out of state for specialized prenatal care. The emergence of hospital-based fetal care programs affords each IDT clinician the opportunity to initiate palliative care throughout the trajectory of care.37 If the baby survives past delivery and beyond the time of the mother’s discharge from the hospital, palliative and hospice care may be provided in the family’s home. Some families may opt for home birth, with care provided by a hospice and midwife team.
Interdisciplinary Team Clinicians
Parents who receive a life-threatening fetal diagnosis may interact with numerous IDT clinicians at multiple sites of care. In fact, each discipline represented in Fig. 37–2 could interact with the family throughout pregnancy, delivery, and the baby’s birth and death. Therefore, it is of utmost importance that a key point person be identified who can facilitate continuity throughout the trajectory of care. As one mother reported to the advanced practice nurse who filled such a role on the palliative care team: “You were our safe, familiar center in the middle of this frightening storm.”
Communication
IDT clinicians should establish and maintain a relationship with the family as the pregnancy continues, supporting the family and facilitating attachment to the baby. Clinicians can help parents anticipate questions from bystanders about the pregnancy. It may be helpful to schedule prenatal visits before or after regular office hours. Some sites may offer separate childbirth education sessions separate from classes for families expecting healthy babies.38
Throughout the EPP, clinicians may find themselves reviewing test results and other prognostic information with parents on multiple occasions. Patience and compassionate listening skills are important. Clinicians should explore with parents how best to provide updates on the baby’s status before, during, and after birth. Parents may worry about how their baby will tolerate labor. Clear expectations should be established about the management plan should fetal distress occur during labor. When the plan is for non-initiation of delivery room resuscitation, good communication among the obstetric, neonatal, and pediatric teams can help make this experience the least obtrusive as possible for families, so that they can cherish the time that they have with their infant. A palliative care order set or protocol can be a helpful communication tool, and should specify orders for vital signs, medications, fluids and/or nutrition, and who should be called to declare death and complete post-mortem documentation (Box 37-1). Staff training and preparation is important, as obstetric and newborn nursery staff who typically care for healthy infants may be unfamiliar with and uncomfortable with neonatal end-of-life care.
BOX 37-1 Sample Palliative Care Order Set for Neonate Following Delivery




Creation of a Birth Plan and Advance Directive
The use of a written birth plan and advance directive can facilitate communication during the EPP.38–40 The co-creation of a birth plan between parents and clinicians provides an opportunity for parents to be actively involved in their baby’s care. As one mother eloquently stated, “this is a special kind of nesting I can do to prepare for my son.”
A well-crafted planning tool should effectively communicate the parents’ wishes for care of the mother during labor and delivery, and should be partnered with advance directives outlining appropriate medical and palliative interventions for the baby. Box 37-2 highlights possible components of a palliative care birth plan and advance directives. It is important to note that this tool is effective only if it is shared, discussed, and readily accessible to all IDT clinicians before the baby’s birth.
BOX 37-2 Components of a Prenatal Palliative Birth Plan and Neonatal Advance Directive
Summarizes parents’ overall goal for their baby
Care of Mother and Baby During Labor and Delivery • Timing, route and location of the baby’s delivery • Management of mother’s pain during labor
Some families may not want to address these issues prior to baby’s death.
Decision Making
The process of decision making in the EPP begins at diagnosis. As reflected in the case study, parents may be offered the option to terminate the pregnancy. Clinicians presenting such options should be clear about any institutional policies related to terminations, such as family counseling, ethical review, or committee approval. Decisions about termination often reflect parents’ moral, ethical and religious views. Data are limited regarding pregnancy outcome following a lethal fetal diagnosis, with two programs reporting 60 percent of parents opting to terminate the pregnancy.37,41 Termination decisions may be further complicated if the family has experienced infertility, or with the diagnosis of a life-threatening condition with one fetus of a multiple pregnancy.
For those parents who choose to continue the pregnancy, subsequent decision making is guided by the certainty of diagnosis, the certainty of prognosis, and the meaning of that prognosis to the parents.39 Together, IDT clinicians and parents work to determine those interventions that are of best interest for the baby, weighing treatment benefits and burdens. There are several congenital conditions for which neonatal resuscitation at birth is not recommended, including anencephaly and trisomy 13. In addition, the American Academy of Pediatrics (AAP)23 and the Neonatal Resuscitation Program42 confirm that resuscitation may be forgone in any scenario if infant survival is unlikely. It is important to note that the number of conditions for which there are clear recommendations for non-resuscitation has decreased steadily over time, as medicine and technology diminish the chance that a disease will be lethal.43
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


