CHAPTER 62 Pelvic inflammatory disease
Introduction
The World Health Organization (WHO) guide to essential practice, ‘Integrating STI/RTI Care for Reproductive Health: Sexually Transmitted and Other Reproductive Tract Infections’, defined reproductive tract infections (RTIs) as a broad term that includes sexually transmitted infections (STIs) as well as other infections that are not sexually transmitted (World Health Organization 2005). Not all STIs are RTIs, a reference to the location of the infection, and not all RTIs are STIs. In most instances, STIs have much more severe health consequences than other RTIs, and the terms ‘STI’ and ‘RTI’ are often used together to highlight the importance of STIs within RTIs.
This chapter will address PID as an upper genital tract infection that may be caused by organisms normally present in the reproductive tract (endogenous), or introduced from the outside during sexual contact (STI) or medical procedures (iatrogenic), and will outline its consequences and management as well as wider global prevention. Readers are also referred to Chapter 63 on non-HIV STIs.
Epidemiology
Epidemiological studies of PID are adversely affected by diagnostic and reporting uncertainties. The symptoms are often subtle and mild, and it is common that many cases of PID are missed because women or healthcare professionals fail to recognize mild or non-specific symptoms and their implications. As there are no simple, safe and specific diagnostic tests for PID, Simms et al (2003) proposed that it was time to rethink its diagnosis.
To complicate matters, adolescent and young adult women are reported to have anxiety surrounding pelvic examination (Millstein et al 1984), and in another study, over half of teens screened for STIs by urine testing and pelvic examination preferred the urine screening (Serlin et al 2002) for evaluating genitourinary (GU) symptoms without undergoing a speculum examination. Such new approaches may encourage young women who fear or otherwise avoid pelvic examinations to receive more timely evaluation, and could also result in access to diagnostic services in settings that do not currently provide them, such as school-based health centres, community centres and detention facilities, enabling clinicians to diagnose and treat many high-risk youth whose infections might otherwise go undetected (Burstein et al 1998, Pack et al 2000).
Estimates of prevalence
Adolescent and young adult women account for nearly half of over 1 million cases of PID reported annually in the USA (Washington and Katz 1991). Chlamydia infection is the most common bacterial STI in the USA, with more than 2.8 million new cases estimated to occur each year (Weinstock et al 2004); this is the most common cause of PID. During 2007, approximately 1.1 million cases of chlamydia were reported to the Centers for Disease Control and Prevention (CDC); more than half of these were in females aged 15–25 years (Centers for Disease Control and Prevention 2009a).The annual incidence and prevalence of STIs is difficult to calculate. The incidence of STIs may be estimated on the bases of nationally notifiable diseases, national surveys, WHO reports and medical literature in this area. There is almost certainly under reporting due to the frequently asymptomatic nature of the disease, and the true annual incidence and prevalence are very likely to be much higher. A recent trend in developed countries highlights a shift in the microbial aetiology of PID, with an increasing role of chlamydia and a decreased role of gonococcal infection (van der Heyden et al 2000). Similarly, PID is now a disease that is mainly diagnosed in primary care or other similar outpatient environments. Since the advent of sensitive molecular amplification tests that permit non-invasive diagnosis of chlamydia, epidemiological evidence suggests that the proportion of chlamydial PID is increasing compared with other causative agents (Hughes et al 2001). There is also evidence that a significant number of chlamydial infections are asymptomatic, which allows silent cross-infection, and if untreated remains infectious in male and female hosts for months. Joyner et al (2002) demonstrated the persistence of chlamydia in 87% of men and women. WHO estimated 89 million new cases of genital chlamydial infections worldwide in 1995 and 92 million in 1999 (Peeling et al 1998, World Health Organization 2001).
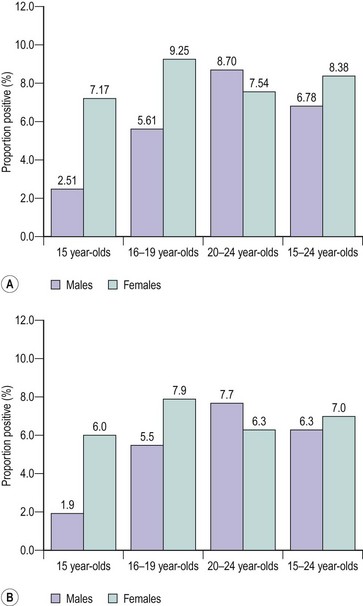
In the UK, STI surveillance systems are based on data from GU medicine clinics and laboratory reports submitted to the Health Protection Agency Centre for Infections. However, this does not take into account the substantial number of relatively asymptomatic STIs that are diagnosed and treated in primary care settings. Simms et al (2006) examined the strengths and weaknesses of the Royal College of General Practitioners’ (RCOG) Weekly Returns Service to determine the incidence of a range of STIs and associated clinical conditions. In their study, data were collated from 78 sentinel general practices in England and Wales between 1994 and 2001, covering a population of approximately 600,000. The authors reported that candidiasis was the most common condition reported in both men and women, followed by PID in women. The mean annual incidences per 100,000 women between 15 and 44 years of age were as follows: PID, 1787; vaginal discharge, 285; non-specific urethritis, 8.2; candidiasis, 4218; Trichomonas vaginalis, 28; genital herpes, 127; and genital warts, 184. Interestingly, the incidence of candidiasis and PID declined over this period in all groups, while the incidence of vaginal discharge doubled in 15–24 year olds over the same period. This decline in the incidence of PID is in marked contrast with the 148% increase in the diagnosis of chlamydial infections made in GU medicine clinics in the same period. The increase in diagnosis may have been brought about by an increase in case ascertainment, the increased availability of diagnostic facilities and an increase in disease incidence, while the decrease in PID probably reflects improved diagnosis and management of the syndrome. The aim of the National Chlamydia Screening Programme (NCSP) since its introduction in England in 2003 has been to control the infection through early detection and treatment of asymptomatic individuals. More than one and a half million (1,673,276) tests were performed on 15–24 year olds by the NCSP between 2003 and the end of July 2009, and a further 376,966 non-NCSP, non-GU medicine tests were reported. Interestingly, the test-positive rate has declined steadily for both men and women since the programme started. The average test-positive rates for screened women and men were 8.38% and 6.78% for 2008–2009, and 7% and 6.3% for the first quarter of 2009–2010, respectively. In both durations, the highest rates were found in women aged 16–19 years and men aged 20–24 years (Figure 62.1). Other risk groups were those reporting behavioural risk factors and certain ethnic groups (National Chlamydia Screening Programme 2009).
Pathogenesis and Pathogens
The main causative agent of PID in the UK is Chlamydia trachomatis. Other less common causes include gonorrhoea, mycoplasma, gardnerella and Gram-negative rods (British Association for Sexual Health and HIV 2005). Trichomonas vaginalis appears to have little, if any, role in the aetiology of PID. Bacterial vaginosis has been associated with PID, and the presence of bacterial vaginosis and leukocytes on vaginal slides is associated with a five-fold risk of PID (von Knorring and Wilson 2007). Other pathogens that should be considered, especially in immigrant women, include tuberculosis and schistosoma. Pelvic and genital tuberculosis is a bloodborne infection. Schistosoma infection should be considered in cases of granulomatous salpingitis (Kameh et al 2004). Actinomycosis is another causative agent of PID, and is often associated with intrauterine contraceptive device (IUCD) use.
Chlamydia
Chlamydia is a Gram-negative obligate intracellular parasite that can cause a variety of disease manifestations in humans. Chlamydia can be defined into different species depending upon its biochemical properties, although molecular analysis has led to further reclassification. In humans, serovars A–C cause conjunctivitis and resultant trachoma, whilst serovars D–K cause urethritis, cervicitis, ophthalmia noenatorum and neonatal pneumonia. LGV serovars produce a specific STI called lymphogranuloma venereum. Chlamydia has many features that are similar to a bacterium. It possesses a cell wall, hence it is sensitive towards penicillin, has the capacity to reproduce RNA and DNA, and is treatable with antibiotics. Unlike bacteria but like viruses, it must infect a host cell to reproduce. These characteristics initially made research difficult, but the application of genetic amplification tests resolved this problem. Chlamydia has a great affinity to adhere to the columnar epithelial cells of the endocervical canal, and also the epithelial cells of the endometrium and fallopian tube. Chlamydia is highly infectious in its extracellular state and consists of particles 0.2–0.4 µm in diameter, known as ‘elementary bodies’. These elementary bodies enter the cell via phagocytosis, but have the capacity to avoid immunological destruction by inhibiting fusion with lysosomes. Over the following 24 h, the elementary bodies expand into larger reticulate bodies. These bodies rapidly divide by a process of binary fission to create several intracellular inclusion bodies, each of which is crammed with thousands of new reticulate bodies. These reticulate bodies condense to form new elementary bodies to complete the replication cycle, and upon lysis of the infected cell, thousands of new highly infectious elementary bodies are released. Host cell destruction is, of course, a byproduct of the replication process, but this is not enough tissue damage to explain the significant upper genital tract damage that occurs with chlamydial infection. This is likely to be due to the host humoral and cell-mediated immune response to infection, and would explain the differences in the effect of the host genetics upon the degree of clinical infection and the long-term sequelae. It is interesting to note that primary infection of chlamydia in monkeys in self-limiting but repeat exposure results in tubal damage, supporting a delayed immune response (Agrawal et al 2007).
Source of entry
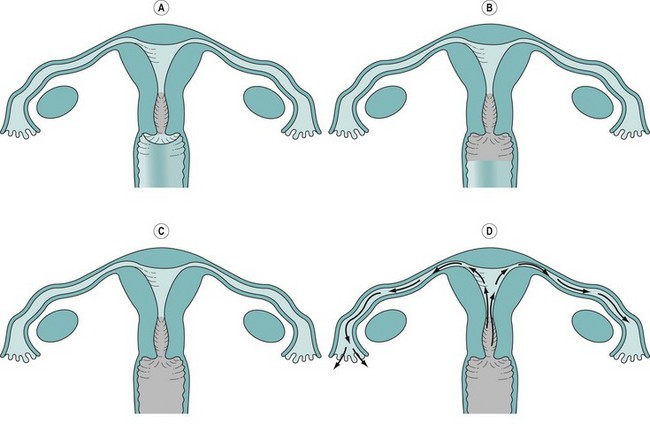
The majority of acute PID are ascending infections through the genital tract to the endocervix, which can act as a reservoir and spread to the endometrium and the peritoneal cavity via the fallopian tubes (Figure 62.2). There is evidence to suggest that the actual degree of symptoms and long-term complications of such infection are greatly dependent upon the type of infection and the host’s immune response. Once infection has gained access to the peritoneal cavity, it can cause a significant inflammatory response including the formation of pus and resultant abscess formation, especially the destructive tubo-ovarian abscess. In addition, pathogens can cause periappendicitis, perisplenitis and perihepatitis. A well-known but inadequately studied phenomenon is the perihepatic adhesions of Fitz–Hughes–Curtis syndrome. It is believed that chlamydia and gonococcus act as primary pathogens disrupting the normal protective barriers of infection, which then allows the clinical infection of other secondary pathogens including endogenous microbes, causing a polyinfection, frequently with anaerobic involvement.
Diagnosis
Symptoms and signs
Even the most experienced reflective clinician may face a dilemma in making a diagnosis of PID, or feel concerned about over- or underdiagnosing PID, primarily due to the lack of good evidence-based diagnostic criteria compounded by its polymicrobial aetiology. Common PID symptoms are outlined in Box 62.1.
The majority of women present with some but not all of these symptoms, which are not pathognomonic and account for the significant differences in determining PID rates among clinicians (Doxanakis et al 2008) and may result in failed treatments. In order to formulate an evidence-based approach to the diagnosis, several authors have attempted to generate a diagnostic scoring system to accept or refute the diagnosis of PID. A frequently used system is that published by Jacobson and Westrom (1969), whereby a diagnosis is made if acute lower abdominal/pelvic pain is accompanied by any two of the following features: abnormal vaginal bleeding, fever, vomiting, menstrual abnormalities, urinary symptoms, proctitis symptoms, marked pelvic tenderness, palpable mass or swelling, or erythrocyte sedimentation rate (ESR) >15 mm/h.
Although this is similar to the current guidelines of the RCOG, it remains a major concern that women with confirmed damaged fallopian tubes have no previous history of PID, mainly due to asymptomatic or atypical disease not being recognized (Sellors et al 1988). Munday’s (2000) comprehensive review of the literature reported that many of the studies undertaken to estimate the accuracy of PID symptoms as a ‘diagnostic test’ had significant methodological flaws. Several used laparoscopy as a gold standard, which unfortunately may not be true, as it was reported to be of limited value with only 64% of suspected PID cases in one series being confirmed at laparoscopy (Sellors et al 1991).
Simms et al (2003) analysed the signs and symptoms of potential PID to generate likelihood ratios, and reported that abnormal vaginal bleeding, fever, vomiting, menstrual irregularity, ongoing bleeding, symptoms of urethritis, marked tenderness of pelvic organs on bimanual palpation, adnexal mass and ESR >15 mm in the first hour did not have significantly high sensitivity or specificity to be clinically valuable, and concluded that there was insufficient evidence to support existing diagnostic criteria for PID.
Current consensus suggests that the positive predictive value of a clinical diagnosis of PID is between 65% and 90% when compared with laparoscopic findings, but this greatly depends upon the population studied (British Association for Sexual Health and HIV 2004). Adnexal tenderness has a particularly high sensitivity of 95%, but a very poor specificity of 22% (Peipert et al 2001).
The CDC factsheet (Centers for Disease Control and Prevention 2009b) indicates that the diagnosis is usually based on clinical findings, and if symptoms are present, a physical examination should be performed and further tests should be undertaken to identify the infection-causing organism. In view of the significant effects and long-term sequelae of untreated PID, it is wise to adopt a low threshold for treatment (Barrett and Taylor 2005) and to initiate early empirical treatment, although there is concern that this may lead to unnecessary treatment of women and there is no evidence to support or refute this strategy (Ross 2001a). With this in mind, clinicians should consider other risk assessments or investigations to improve diagnostic accuracy.
Risk assessment
Risk factors for STIs and PID are the same. In a longitudinal study, it was found that 39% of women with laparoscopically diagnosed PID were found to be infected with chlamydia and 14% with gonorrhoea (Bevan et al 1995). It is important to take a comprehensive sexual history from a patient with suspected PID. Risk factors include multiple sexual partners, lack of barrier contraception, young age and lower socioeconomic group. There is good evidence that anything that disrupts the cervical mucous barrier is a risk factor for PID. This includes uterine instrumentation, termination of pregnancy and insertion of an IUCD. There is significant evidence to support the fact that there are different levels of host susceptibility towards the development of PID, whereby polymorphism of mannose-binding lectin, an important component of the innate immune system and protector against chlamydial infection, may affect the extent of tubal damage in cases of chlamydial infection (Sziller et al 2008).
Evidence-Based Management
Investigations
Specific tests
Several tests may be employed for the diagnosis of PID, including microbiological swabs (endocervical, urinary, high and low vaginal swabs), inflammatory markers (C-reactive protein, ESR and differential white cell counts) and biophysical tests [transvaginal ultrasound scanning, Doppler scanning and magnetic resonance imaging (MRI) of the pelvis]. Microbiological tests remain the principal approach for the diagnosis of gonococcal and chlamydial infections, although the PID rate caused by the former is decreasing. Chlamydial tests have included cell culture, antibody tests and, more recently, nucleic acid amplification tests (NAAT), which allow greater accuracy at a relatively low cost. A recent meta-analysis suggested that pooled sensitivities for ligase chain reaction, polymerase chain reaction, gene probe and enzyme immunoassay of urine specimens were 96.5%, 85.6%, 92% and 38%, respectively, while on cervical swabs, the corresponding sensitivities were for PCR, gene probe and EIA 88.6%, 84% and 65%, respectively (Watson et al 2002). With any test, it is important to remember that the absence of lower genital tract infection does not exclude PID (Royal College of Obstetricians and Gynaecologists 2009).



