Chapter 71 Pediatric Pain Management
Definition and Categories of Pain
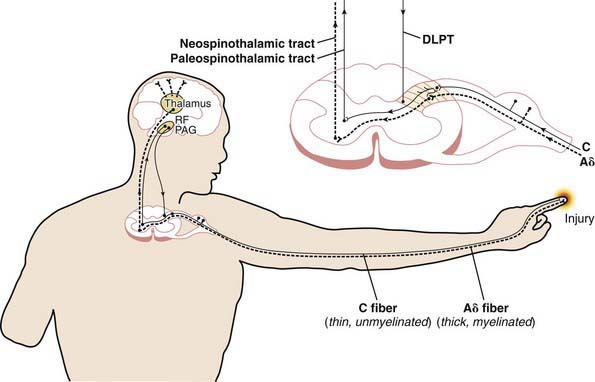
Table 71-1 specifies important pain categories commonly treated (somatic, visceral, and neuropathic) and defines the elements and characteristics of nociception, the peripheral physiologic aspect of pain perception (Fig. 71-1). Nociception refers to how specialized fibers (largely but not exclusively the A delta and C fibers) in the peripheral nervous system transmit nerve impulses (often originating from peripheral mechanoreceptors and chemoreceptors) through synapses in the spinal cord’s dorsal horn through (but not exclusively through) the spinothalamic tracts to the brain’s higher centers, where nociception is converted to pain with all of its cognitive and emotional ramifications.
Table 71-1 PAIN CATEGORIES AND CHARACTERISTICS
| PAIN CATEGORY | DEFINITION AND EXAMPLES | CHARACTERISTICS |
|---|---|---|
| Somatic | Pain resulting from injury to or inflammation of tissues (skin, muscle, tendons, bone, joints, fascia, vasculature, etc.) | |
| Visceral | Aching and cramping; nonpulsatile; poorly localized (e.g., appendiceal pain perceived around umbilicus) or referred to distant locations (e.g., angina perceived in shoulder) | |
| Neuropathic | Pain resulting from injury to, inflammation of, or dysfunction of the peripheral or central nervous systems. | Spontaneous; burning; lancinating or shooting; dysesthesias (pins and needles, electrical sensations); hyperalgesia (amplification of noxious stimuli); hyperpathia (widespread pain in response to a discrete noxious stimulus); allodynia (pain in response to nonpainful stimulation); pain may be perceived distal or proximal to site of injury, usually corresponding to innervation pathways (e.g., sciatica) |
The Assessment and Measurement of Pain in Children
Age-Specific and Developmentally Specific Measures
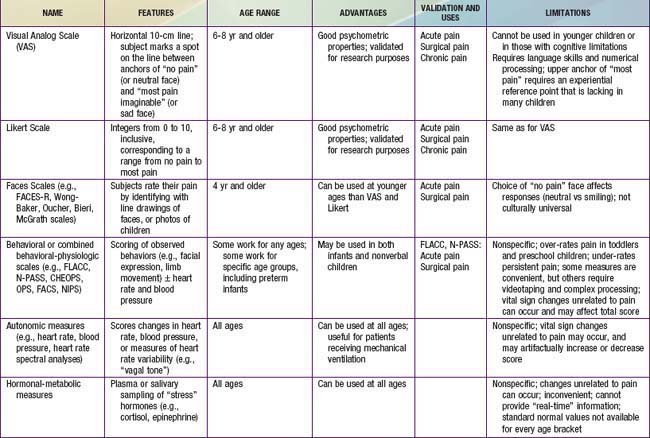
Because infants, young children, and nonverbal children cannot express the quantity of pain they experience, several pain scales have been devised in an attempt to quantify pain in these populations (Fig. 71-2; Table 71-2).
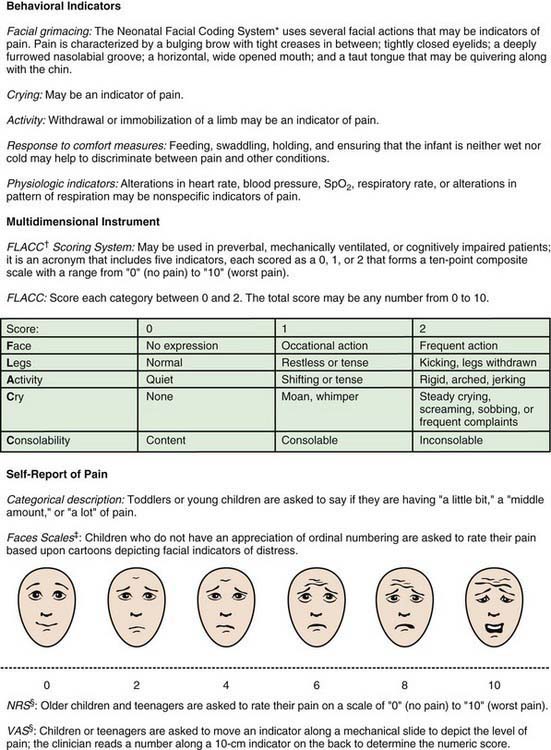
Figure 71-2 Clinically useful pain assessment tools.
(Adapted from Burg FD, Ingelfinger JR, Polin RA, et al, editors: Current pediatric therapy, ed 18, Philadelphia, 2006, Saunders/Elsevier, p 16; and Hicks CL, von Baeyer CL, Spafford P, et al: The Faces Pain Scale—revised: toward a common metric in pediatric pain measurement, Pain 93:173–183, 2001.)
The Older Child
Children 3-7 yr old become increasingly articulate in describing the intensity, location, and quality of pain. Pain is occasionally referred to adjacent areas; referral of hip pain to the leg or knee is common in this age range. Self-report measures for children this age include using drawings, pictures of faces, or graded color intensities. Children age 8 yr and older can usually use verbal scales or visual analog pain scales (VASs) accurately (see Fig. 71-2). Verbal numerical ratings are preferred and considered the gold standard; valid and reliable ratings are for children 8 yr and older. The Numerical Rating Scale (NRS) consists of numbers from 0 to 10, in which 0 represents no pain and 10 represents very severe pain. There is debate about the label for the highest pain rating, but the current agreement is NOT to use the worst pain possible, because children can always imagine a greater pain. In the USA, regularly documented pain assessments are required for hospitalized children and children attending outpatient hospital clinics and emergency departments. Pain scores do not always correlate with changes in heart rate or blood pressure.
The Treatment of Pain
Both pharmacologic and nonpharmacologic approaches to pain management should be considered for all pain treatment plans. Many simple interventions designed to promote relaxation and patient control can be expected to work synergistically with pain medications for optimal relief of pain and related distress. Psychologic and developmental comorbidities affect the child’s experience of pain and ability to tolerate and cope with it. Thus, it is important to assess a child for evidence of situational anxiety and/or anxiety disorders, such as generalized anxiety disorder, post-traumatic stress disorder, social anxiety, separation anxiety, panic disorder, and obsessive-compulsive disorder (Chapter 23). Depression assessment should include current suicidal ideation and intent as well as past history of suicidal gestures or attempts (Chapters 24 and 25). Developmental assessment includes evaluating for specific learning disorders, Asperger disorder, and evidence of pervasive developmental disorders in general, including autism spectrum disorders (Chapter 28). All psychologic and developmental comorbidities should be determined and addressed, to adequately treat the child in pain or to reduce the risk of the child’s developing ongoing pain after surgery, trauma, or even invasive medical procedures.
Pharmacologic Treatment of Pain
Acetaminophen, Aspirin, and Nonsteroidal Anti-Inflammatory Drugs
Acetaminophen (APAP) and nonsteroidal anti-inflammatory drugs (NSAIDs) have replaced aspirin as the most commonly used antipyretics and oral, nonopioid analgesics (Table 71-3).
Table 71-3 COMMONLY USED NONOPIOID MEDICATIONS
| MEDICATION | DOSAGE | COMMENT(S) |
|---|---|---|
| Acetaminophen | Little anti-inflammatory action; no antiplatelet or adverse gastric effects; over-dosing can produce fulminant hepatic failure | |
| Aspirin | Anti-inflammatory; prolonged antiplatelet effects; may cause gastritis; associated with Reye’s syndrome | |
| Ibuprofen | 8-10 mg/kg PO q6h | Anti-inflammatory; transient antiplatelet effects; may cause gastritis; extensive pediatric safety experience |
| Naprosyn | 5-7 mg/kg PO q8-12h | Anti-inflammatory; transient antiplatelet effects; may cause gastritis; more prolonged duration than that of ibuprofen |
| Ketorolac | Loading dose 0.5 mg/kg, then 0.25-0.3 mg/kg IV q6h to a maximum of 5 days; maximum dose 30 mg loading with maximum dosing of 15 mg q6h | Anti-inflammatory; reversible antiplatelet effects; may cause gastritis; useful for short-term situations in which oral dosing is not feasible |
| Celecoxib | 3-6 mg/kg PO q12-24h | Anti-inflammatory; no antiplatelet or gastric effects; cross-reactivity with sulfa allergies |
| Choline magnesium salicylate | 10-20 mg/kg PO q8-12h | Weak anti-inflammatory; lower risk of bleeding and gastritis than with conventional NSAIDs |
| Nortriptyline, amitriptyline, desipramine | 0.1-0.5 mg/kg PO qhs | For neuropathic pain; facilitates sleep; may enhance opioid effect; may be useful in sickle cell pain; risk of dysrhythmia in prolonged QTc syndrome; may cause fatal dysrhythmia in overdose; FDA says agents may enhance suicidal ideation |
| Gabapentin | 100 mg bid or tid titrated to up to 3600 mg/24h | For neuropathic pain; associated with sedation, dizziness, ataxia, headache, and behavioral changes |
| Quetiapine, risperidone, chlorpromazine, haloperidol | Quetiapine: 6.25 or 12.5 mg PO qd (hs); may use q6hr prn acute agitation with pain. Escalate dose to 25 mg/dose if needed. | Useful when arousal is amplifying pain; often used when patient first starting SSRI and then weaned after at least 2 wk; check for normal QTc before initiating; side effects include extrapyramidal reactions (diphenhydramine may be used to treat) and sedation; in high doses, can lower the seizure threshold |
| Fluoxetine | 10-20 mg PO qd (usually in morning) | SSRI for children with anxiety disorders in which arousal amplifies sensory signaling; useful in PDD spectrum disorders in very low doses; best to use in conjunction with psychiatric evaluation |
| Sucrose solution via pacifier or gloved finger | Allow 2 min before starting procedure; analgesia may last up to 8 min; the dose may be repeated once |
FDA, U.S. Food and Drug Administration; IV, intravenous(ly): NSAIDs, nonsteroidal anti-inflammatory drugs; PDD, pervasive developmental disorder; PDR, Physicians’ Desk Reference; QTc, corrected QT interval on an electrocardiogram; SSRI, selective serotonin reuptake inhibitor.
Acetaminophen, a generally safe, nonopioid analgesic and antipyretic, has the advantage of rectal and oral routes of administration, is expected to be available soon also as an intravenous (IV) preparation in the USA, as it is now in Europe. Acetaminophen is not associated with the gastrointestinal or antiplatelet effects of aspirin and NSAIDs, making it a particularly useful drug in patients with cancer. Unlike aspirin and NSAIDs, acetaminophen has only mild anti-inflammatory action. Acetaminophen toxicity can result from either, large single doses or cumulative, excessive dosing over days or weeks (Chapters 58 and 355). A single, massive overdose overwhelms the normal glucuronidation and sulfation metabolic pathways in the liver, whereas long-term overdosing exhausts supplies of the sulfhydryl donor glutathione, leading to alternative cytochrome P-450 catalyzed oxidative metabolism and the production of the hepatotoxic metabolite N-acetyl-p-benzoquinone imine (NAPQI). Toxicity manifests as fulminant hepatic necrosis and failure in infants, children, and adults. Drug biotransformation processes are immature in neonates, very active in young children, and somewhat less active in adults. Young children are more resistant to acetaminophen-induced hepatotoxicity than adults as a result of metabolism differences: Sulfation predominates over glucuronidation in young children, leading to a reduction in NAPQI production.
Aspirin (ASA) is indicated for certain rheumatologic conditions and for inhibition of platelet adhesiveness, as in the treatment of Kawasaki disease. Concerns about Reye syndrome have resulted in a substantial decline in pediatric aspirin use (Chapter 349).
Adverse effects of NSAIDs are uncommon, but they may be serious when they occur. They include gastritis with pain and bleeding; decreased renal blood flow that may reduce glomerular filtration and enhance sodium reabsorption, in some cases leading to tubular necrosis; hepatic dysfunction and liver failure; and inhibition of platelet function. Although the overall incidence of bleeding is very low, NSAIDs should not be used in the child with a bleeding diathesis or at risk for bleeding or when surgical hemostasis is a prominent concern, such as after tonsillectomy. Renal injury from short-term use of ibuprofen in euvolemic children is quite rare; the risk is increased by hypovolemia or cardiac dysfunction. The safety of both ibuprofen and acetaminophen for short-term use is well established (see Table 71-3).
Opioids
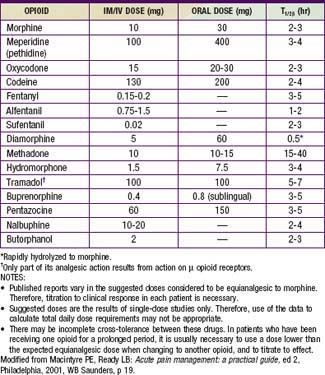
Opioids are analgesic substances either derived from the opium poppy (opiates) or synthesized to have a similar chemical structure and mechanism of action (opioids). The older, pejorative term narcotics should not be used for these agents, because it connotes criminality and lacks pharmacologic descriptive specificity. Opioids are administered for moderate and severe pain, such as acute postoperative pain, sickle cell crisis pain, and cancer pain. Opioids can be administered by the oral, rectal, oral transmucosal, transdermal, intranasal, IV, epidural, intrathecal, subcutaneous, or intramuscular route. Historically, infants and young children have been underdosed with opioids for fear of significant respiratory side effects. With proper understanding of the pharmacokinetic and pharmacodynamics of opioids, children can receive effective relief of pain and suffering with a good margin of safety (Tables 71-4 to 71-7).
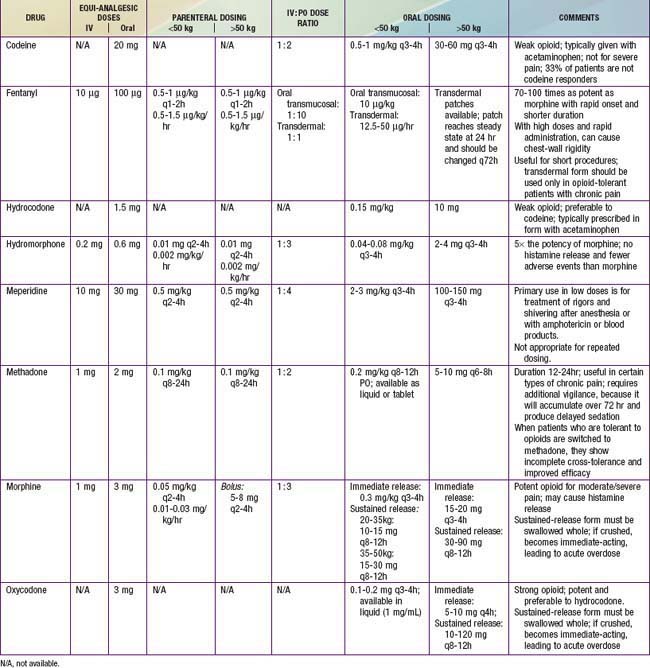
Table 71-5 PRACTICAL ASPECTS OF PRESCRIBING OPIOIDS
Table 71-6 MANAGEMENT OF OPIOID-INDUCED ADVERSE EFFECTS
* Avoid in patients taking monoamine oxidase inhibitors.
† May be associated with extrapyramidal side effects, which may be more commonly seen in children than in adults.
Modified from Burg FD, Ingelfinger JR, Polin RA, et al, editors: Current pediatric therapy, ed 18, Philadelphia, 2006, Saunders/Elsevier, p 16.
Optimal use of opioids requires proactive and anticipatory management of side effects (see Table 71-6). Common side effects include constipation, nausea, vomiting, urinary retention, and pruritus. The most common, troubling but treatable side effect is constipation. Stool softeners and stimulant laxatives should be administered to most patients receiving opioids for more than a few days. Constipation also remains a problem with long-term opioid administration. A peripherally acting opiate µ receptor antagonist, methylnaltrexone, promptly and effectively reverses opioid-induced constipation in patients with chronic pain who are receiving opioids daily. The side effect of nausea typically subsides with long-term dosing, but it may require treatment with antiemetics, such as a phenothiazine, butyrophenones, antihistamines, or a serotonin receptor antagonist such as ondansetron or granisetron. Pruritus and other complications during patient-controlled analgesia (PCA) with opioids may be effectively managed by low-dose IV naloxone (see Table 71-6).
One of the potent barriers to effective management of pain with opioids is the unrealistic fear of addiction held by many prescribing pediatricians and parents. Pediatricians should understand the phenomena of tolerance, dependence, withdrawal, and addiction (see Table 71-5) and should know that the rational short- or long-term use of opioids in children does not lead to a predilection or risk of addiction in a child not otherwise at risk by virtue of genetic background and social milieu. It is important for pediatricians to realize that even patients with recognized substance-abuse diagnoses are entitled to effective analgesic management, which often includes the use of opioids. When there are legitimate concerns about addiction in a patient, then safe, effective opioid pain management is often best managed by specialists in pain management and/or addictionology.
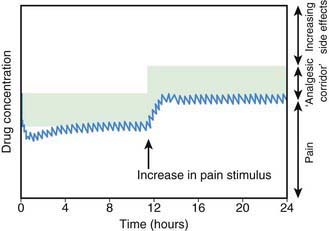
There is no longer a reason to administer opioids by intramuscular injection. Continuous IV infusion of opioids is one, effective option that permits more constant plasma concentrations and clinical effects than intermittent IV bolus dosing, without the pain associated with intramuscular injection. The most common approach in pediatric centers is to administer a low-dose basal opioid infusion, while permitting patients to use a PCA device to titrate the dosage above the infusion (Chapter 70; Fig. 71-3). Compared with children given intermittent intramuscular morphine, children using PCA reported better pain scores. PCA has several other advantages: (1) dosing can be adjusted to account for individual pharmacokinetic and pharmacodynamic variation and for changing pain intensity during the day, (2) psychologically, the patient is more in control, actively coping with the pain, (3) overall opioid consumption is lower, (4) fewer side effects occur, and (5) patient satisfaction is generally much higher. Children as young as 5-6 yr can effectively use PCA. The device can be activated by parents or nurses—the latter practice known as PCA-by-proxy (PCA-P); PCA-P produces analgesia in a safe, effective manner for children who cannot activate the PCA demand button themselves because they are too young or intellectually or physically impaired. PCA overdoses occur when well-meaning, inadequately instructed parents pushed the PCA button in medically complicated situations with or without the use of PCA-P, highlighting the need for patient and family education, the use of protocols, and adequate nursing supervision.