31 Otitis
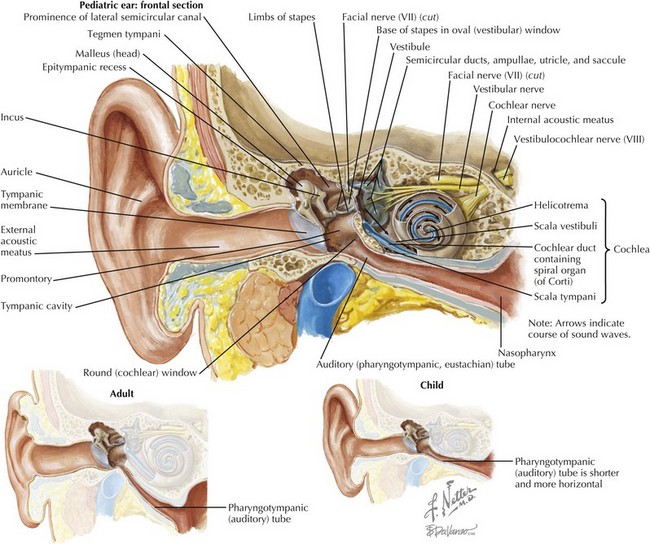
To first review basic anatomy, the ear is divided into three parts: the outer, middle, and inner ear. The outer ear consists of the auricle and ear canal up to the tympanic membrane (TM). The middle ear is bounded by the TM and the round window. The middle ear contains three bones that conduct sound—the malleus, the incus, and the stapes—and the Eustachian (pharyngotympanic) tube that connects the middle ear cavity to the pharynx. The inner ear contains the cochlea and semicircular canals (Figure 31-1).
Otitis Externa
Clinical Presentation
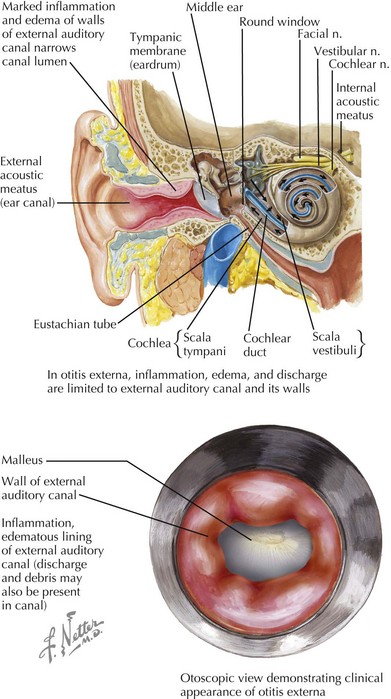
In AOE, the physical examination is critical in diagnosis. Debris and cerumen must be cleared from the canal to ensure accurate otoscopy of the TM as well as to improve the ability of topical treatment to reach the area of infection. The hallmark sign of AOE is tenderness of the tragus or the pinna when manipulated. The clinician will see diffuse edema and erythema of the canal, possibly with otorrhea or other debris present (Figure 31-2). The TM may be erythematous, but this should not imply a definite diagnosis of otitis media. On pneumatic otoscopy, if there is normal movement of the TM without visible effusion, the erythema may be attributed to the AOE.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


