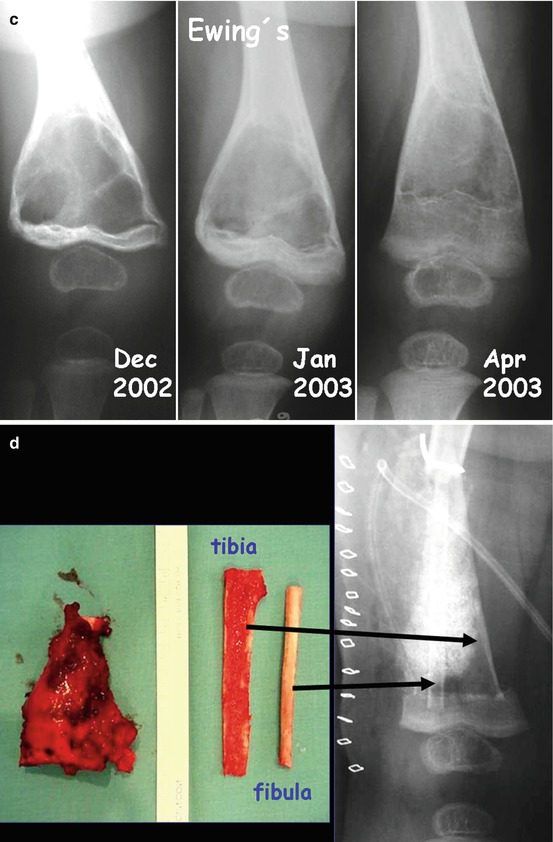
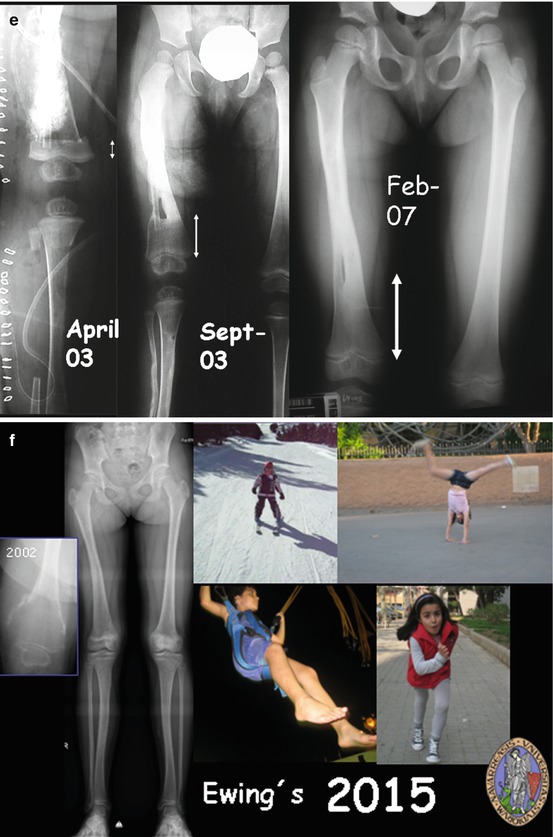
Fig. 13.1
(a) Ewing’s sarcoma in the distal metaphysis of the femur of a 9-month-old baby. MRI shows is in contact with the physis. Most of our colleagues dealing with bone tumors would advise an amputation. (b, c) Neoadjuvant treatment was very succesful. Note the new bone formation from the distal femur growth plate. (d, e) Resection was performed through metaphyseal and diaphyseal osteotomies in order to preserve the joint. Autografts from ipsilateral fibula and tibia were used for reconstruction. (f) Follow-up: 13 years later, limb function is excellent (Reproduction from San-Julian et al. [14])
Fig. 13.2
(a) Osteosarcoma in the distal metaphysis of the femur of 8-year-old girl. (b) She started chemotherapy elsewhere and suffered a pathological fracture. (c) After neoadjuvant chemotherapy in our center. Note the growth in the distal femur growth plate that has displaced the tumor to the diaphysis. (d) Resection and reconstruction with an allograft. Good healing was obtained
13.2 Intra-epiphyseal Osteotomy
Prior to the first publications of our work, the possibility of preservation of the epiphysis in metaphyseal bone tumors was apparently largely overlooked, and alternative techniques, such as intra-epiphyseal osteotomy [9], have only been suggested subsequently. We have used intra-epiphyseal osteotomy in some cases, in which epiphysis could be preserved but physeal distraction was contraindicated (Figs. 13.3 and 13.4).
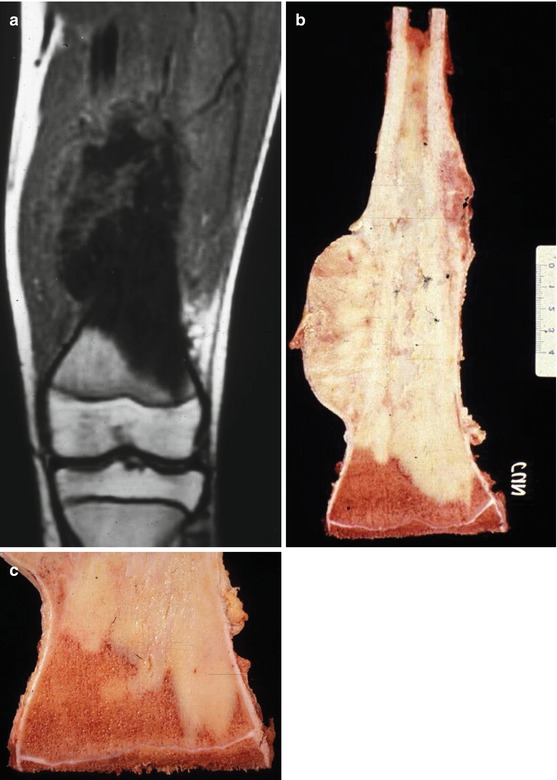
Fig. 13.3
(a) Osteosarcoma in the distal metaphysis of the femur of a 16-year-old boy. MRI shows the tumor in contact with the physis. This patient was treated in 1987. (b, c) Intra-epiphyseal osteotomy was performed in order to preserve the joint. Note that the growth plate is very thin
Fig. 13.4
(a, b) Osteosarcoma in the proximal metaphysis of the tibia of a 17-year-old boy. The tumor is in contact with the growth plate. (c) After careful consideration of epiphysiolysis before resection, we chose intra-epiphyseal osteotomy in view of the age of the patient. (d, e) Reconstruction with an intercalary allograft stabilized with both a plate and a nail
In the more recent reports of intra-epiphyseal osteotomy [2, 6–8, 10–12], the technique has been used mainly in proximal tibia locations. Tumor involvement of the physis is assessed by preoperative MRI. If intra-epiphyseal osteotomy is indicated, it is done under X-ray control in order to include the growth plate in the resected specimen. The residual epiphyseal bone segment is less than 2 cm thick and reconstruction is by a combination of vascularized fibula and allograft [3]. Authors report that local recurrence has not been observed to occur in the retained epiphysis [2, 13]. Other authors [1, 5] have employed metallic implants for reconstruction of the intercalary region, but follow-up is not yet long enough to know the long-term results with such implants. An epiphyseal osteotomy is fixed with small fragment screws.
In our opinion, the advantages of physeal distraction over intra-epiphyseal osteotomy are:
1.
Get Clinical Tree app for offline access

Safety. The growth plate is not a flat surface – it has indentations and protuberances (Figs. 13.5 and 13.6) – and consequently intra-epiphyseal osteotomy could leave bits of tumor.

Fig. 13.5




(a) Because of the morphology of the growth plate, intra-epiphyseal osteotomy could leave tumor cells in the hollows of the surface. (b) Experimental epiphysiolysis in a lamb. Note the undulate appearance of the growth plate
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree