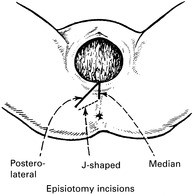
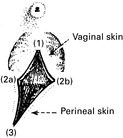
Making an incision in the perineal body at the time of delivery.
Indications
Types of Incision
Technique

Repair
FORCEPS DELIVERY
Indications for the use of forceps
Conditions for forceps delivery
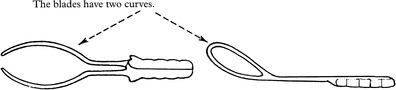
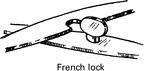
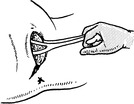
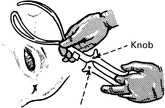
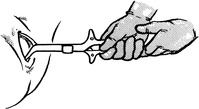
OBSTETRIC FORCEPS


Low Forceps
Mid Forceps
Wrigley’s Forceps

Anderson’s (Simpson’s) Forceps

Kielland’s Forceps




FORCEPS DELIVERY
Preparations
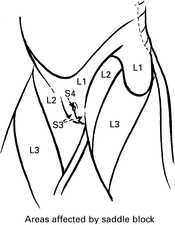
Anaesthesia

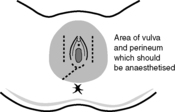
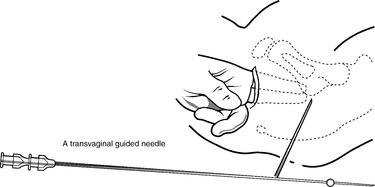
Pudendal Nerve Block
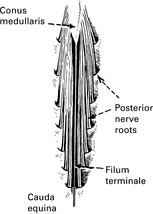
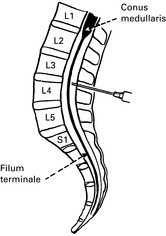
Physiology of Spinal Anaesthesia
Circulatory Effects
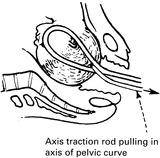
LOW FORCEPS DELIVERY





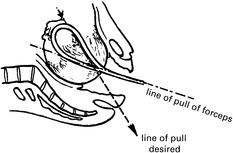
MID FORCEPS DELIVERY




DELIVERY WITH KIELLAND’S FORCEPS







![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree