chapter 13 Neurological Examination
The Logic Behind the Approach
At each phase of the assessment, try to determine the site of the lesion. Doing so makes it easier to compile a list of differential diagnoses or hypotheses. As an initial approach, divide neurological disorders into upper motor neuron lesions (UMNLs) and lower motor neuron lesions (LMNLs). The major features of each are listed in Table 13–1. Remember that some children, such as those with leukodystrophies, may have a mixture of both UMNL and LMNL signs, and localizing the problem to a single focal lesion in such patients is not possible. In addition, children with disorders of the cerebellum or basal ganglia do not have UMNL signs.
TABLE 13–1 Signs of Upper and Lower Motor Neuron Lesions
| Parameters | Upper Motor Neuron Lesions: Central Nervous System Dysfunction* | Lower Motor Neuron Lesions: Peripheral Nervous System Dysfunction† |
|---|---|---|
| Intellect | Deficits may be found with cortical abnormalities | Normal |
| Cranial nerves | Abnormalities usually reflect brainstem involvement but may indicate a neuropathy | May be involved |
| Power | Slightly decreased, although movement more severely impaired because of altered tone | Markedly reduced; neuromuscular junction disease associated with fatigue |
| Tone | Increased (spasticity) with lesions affecting pyramidal pathways; rigidity seen with extrapyramidal disease | Reduced (floppy or hypotonic) |
| Coordination | Impaired when cerebellum or its connections are involved | May be hindered by weakness |
| Reflexes | Hyperactive in pyramidal dysfunction; plantar stimulation results in an extensor response (Babinski) in the great toe | Difficult to elicit |
| Sensation | Usually intact, but spinal cord gives a sensory level that is in a dermatomal distribution | Impaired with lesions that affect the nerve |
| Fasciculations | Present with anterior horn cell disease but occasionally also found with neuropathies |
* Involve intracranial contents, brainstem, or spinal cord.
† Involve intracranial horn cells, nerves, neuromuscular junction, or muscles.
Obtaining the History
When combined with a hands-off observation, the history usually provides the diagnosis (see Chapter 1). The physical examination rarely reveals previously unsuspected findings.
The school-aged child
A brief but detailed history of the pregnancy is essential. Most mothers remember the pregnancy and birth in vivid detail and often have unfounded fears related to it (see Chapter 1). Reassuring a mother that the cough medicine she took during the third trimester was not the cause of her baby’s meningomyelocele may relieve anxiety. Similarly, if a child has been discharged from the neonatal unit at the same time as his/her mother, it is extremely unlikely that significant perinatal problems occurred.
Observation
The school-aged child
Power
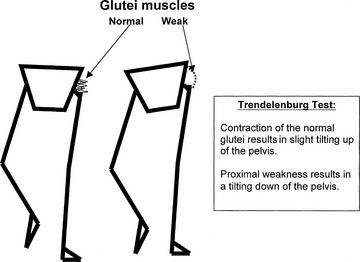
Proximal leg weakness, seen in myopathies such as muscular dystrophy, may be apparent if the child walks with a waddling gait. The Trendelenburg sign indicates a weakness of the hip abductors and is reflective of proximal weakness. Normally, when the child stands on one leg, the glutei contract, and the other side of the pelvis is tilted slightly upward. When the child has proximal weakness, the glutei are not sufficiently strong, and the other hip tilts downward. To maintain balance, the trunk leans over toward the side of the lesion; this is called the Trendelenburg sign (Fig. 13–1). Weakness and wasting of the hand muscles are more likely to indicate a neuropathy. Note that proximal weakness indicates a myopathy, and distal weakness indicates a neuropathy. Myotonic dystrophy, a dominantly inherited myopathy characterized by distal weakness and the inability to relax the muscles, is essentially the only major exception to this rule in childhood. During the period of observation, look for any asymmetry in limb movements. (See Video 13-3 on Student Consult.)
Coordination
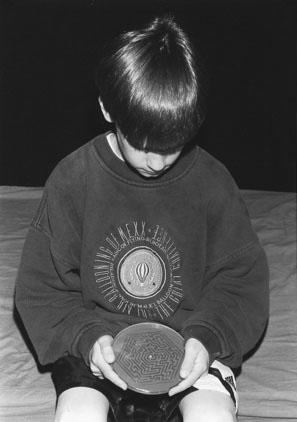
For older children, I use a challenging maze puzzle, which is an excellent test of coordination (Fig. 13–2). Cerebellar lesions affect the ipsilateral limb.
Reflexes and Sensation
Reflexes and sensation are examined during the physical examination, which is described later.
Abnormal Movements
The more common abnormal movements are described here:
The preschool-aged child
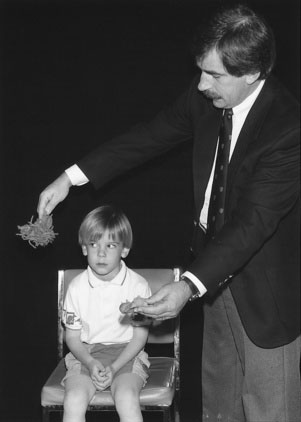
In the younger child, a period of hands-off observation should always be the first part of the physical examination. I give puzzles, a pencil, and paper to the younger child. Giving children toys allows you to observe the youngster’s manual dexterity, coordination, developmental competence, and handedness (Fig. 13–3). Observe the parent-child interaction closely. You may detect discipline problems at this stage. Drawings also reveal visual-spatial abilities, fine motor skills, and the child’s level of attention. Allowing the child to play also provides important undisturbed time with the parents as you take the history.

The Physical Examination
The school-aged child
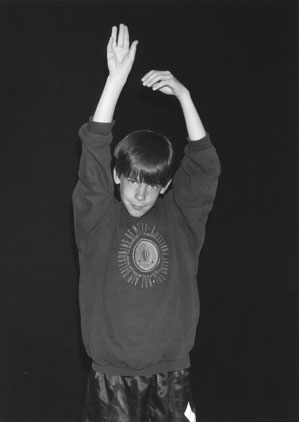
Holding the extended and supinated arms in front of the body also tests for weakness. Children with a mild weakness will be unable to maintain this position, and the arms tend to drift downward, flex at the elbow, and pronate (Fig. 13–4).
Cortical Function
School-aged and preschool-aged children
Assess each cortical area in turn.
Temporal Lobes
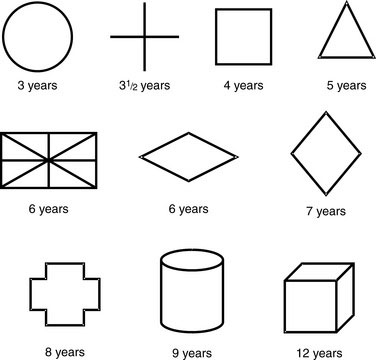
Temporal lobe impairment may cause personality changes similar to those seen with frontal lobe damage. Language is also represented in this lobe, and lesions of the superior and middle gyri cause Wernicke aphasia, characterized by an impaired comprehension of word elements. The ability to read, write, and understand speech may be altered. If the nondominant temporal lobe is involved, the child has a distorted perception of spatial relationships and a change in musical appreciation. Test for alterations in spatial perception by asking the child to copy geometric designs. Age-appropriate designs are shown in Figure 13–5. Bilateral involvement of the hippocampus interferes with learning. Temporal lobe injury also may produce psychotic aggressive behavior. Visual symptoms are usually represented by a homonymous superior quadrantanopia.
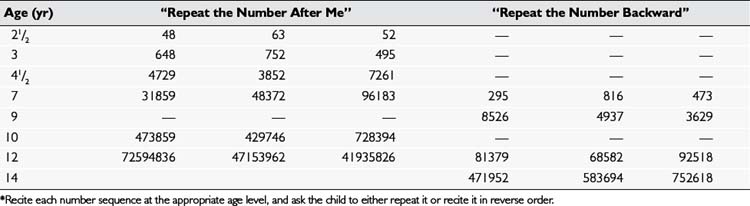
Memory deficits may be seen with a temporal lobe dysfunction. You can test a child’s immediate recall by reciting number sequences and having the child repeat them after you, either in the same order or in reverse; Table 13–2 gives examples of age-appropriate number sequences for this test.
Cranial Nerve II (Optic)
Always separately test each eye (see Chapter 8), and divide the examination into the following four parts.
Visual fields
The Preschool-Aged Child
For the younger child, test the visual fields by distracting him or her with a toy in front while bringing a red toy from behind the youngster into the peripheral field of vision (Fig. 13–6). The child with normal vision should respond as soon as the toy reaches a line perpendicular to the outer canthus of the eye.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


