26
Neoplasia
Chapter map
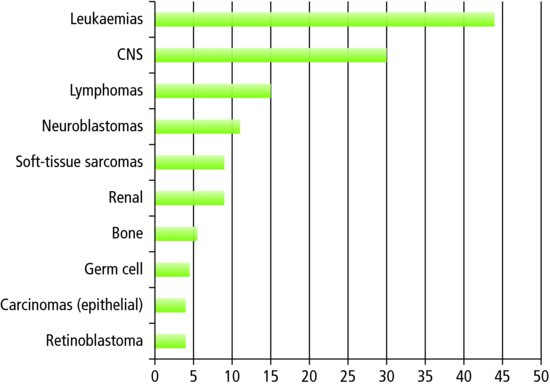
Malignant disease is the second most common cause of death in childhood after accidents. Leukaemia has the highest incidence (Figure 26.1). With 1200 newly diagnosed UK cases a year, a child has a 1 in 600 chance of developing a malignancy before reaching adulthood. There has been steady improvement in outcome over the past decades due to ongoing treatment development, and the fact that most patients are entered into multicentre clinical trials. For the 0-14 year age-group, 5-year survival is 80% in Europe and the USA. Cure rates vary by tumour type, from around 60% for acute myeloid leukaemia, neuroblastoma and CNS tumours, to above 90% for Hodgkin’s lymphoma.
26.3 Central nervous system tumours
26.5 Wilms tumour (nephroblastoma)
26.7 Treatment of childhood malignancy
Figure 26.1 Incidence of childhood malignancy in Europe. New cases per million population. Source: adapted from data in Kaatsch (2010).
- Leukaemia
- Lymphoma
- CNS tumours.
The relative frequency of different types of malignancy varies through childhood (Figure 26.2). In contrast to adult disease, childhood epithelial malignancies (e.g. carcinoma of the lung and gastrointestinal tract) are very rare. In children, the prognosis for malignancy is better than in adults (Table 26.1). Some genetic conditions increase the lifetime risk of cancer (e.g. Down syndrome, neurofibromatosis).
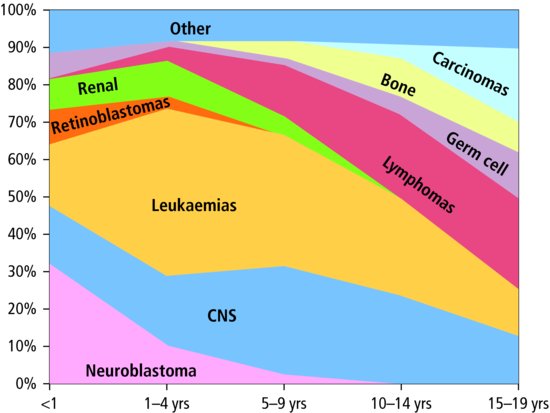
Table 26.1 5-year survival rates (%) for childhood malignancy
| 5 year survival | |
| Malignancy | rate (%) |
| Hodgkin’s lymphoma | 95 |
| Wilm’s tumour | 84 |
| Astrocytoma | 83 |
| Acute lymphoblastic leukaemia | 84 |
| Osteosarcoma | 68 |
| Neuroblastoma | 73 |
| All childhood malignancy | 80 |
Early diagnosis improves outcomes. However, many of the initial presenting signs and symptoms are relatively common in the general population, so care is needed, and a high index of suspicion (Table 26.2). Early review, further investigation, or urgent referral should be considered.
Table 26.2 Common symptoms – when to worry
| Malignancy unlikely* | Malignancy more likely | |
| Lymphadenopathy | Smooth, mobile, <2 cm Cervical or small inguinal Well child | Hard, craggy, tethered Bruising, pallor, fever Hepatosplenomegaly |
| Headaches | Typical migraine or stress headache Longstanding in older child No neurological signs or symptoms No other concerning symptoms (see section on central nervous system tumours below) | Present on waking Worse on coughing/sneezing Recent onset, worsening or persistent Any neurological signs/symptoms Any other concerning symptoms |
| Aches and pains | Vague, difficult to localize Well child No local signs | Localized pain Local signs (e.g. swelling and tenderness) Unusual pain (e.g. back pain in a toddler) |
| *Note that there may be other differential diagnoses for these symptoms. | ||
26.1 Acute leukaemia
Leukaemia is characterized by the malignant proliferation of abnormal white cells (blasts) within the bone marrow. Acute lymphoblastic leukaemia accounts for 85% of cases. It is more common in boys and has a peak incidence between 2 and 5 years of age.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


