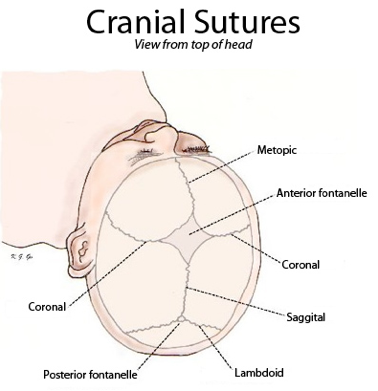
Fig. 1
Cranial sutures and fontanelles. The soft spots between the cranial sutures are the anterior and posterior fontanelles. The fontanelles close by age 18-months-old (Source: Adapted from xxjamesxx under Creative Commons Attribution-Share Alike Unported license as published on https://upload.wikimedia.org/wikipedia/commons/5/5f/Sutures_from_top.png. Downloaded 1 Jan 2014)
{kind=link}
(f)
Temperature control:
(i)
Infants and newborns have a large surface area to volume ratio that allows for greater heat loss. They also lack significant amounts of insulating body fat. If proper precautions are not taken, small infants are at profound risk for heat loss from conduction, convection, evaporation, and radiation. Important thermoregulatory mechanisms are immature and inefficient in the preterm and small infant. For example, brown fat which is produced during the third trimester is vital for thermogenesis. This lack of brown fat in infants born preterm impedes the infant’s innate ability to mount an adequate response to cold stress. In addition, small infants have a limited or absent ability to shiver. Since infants have immature thermoregulation, close attention to maintaining euthermia should be an essential component in the care of the postoperative patient.
3.
Transition of care from the operative /anesthetic setting to the neonatal or pediatric ICU:
(a)
The Joint Commission estimates that 80 % of serious medical errors involve miscommunication during care transitions. Miscommunication was the leading root cause of sentinel events reported to the commission between 1995 and 2006. The majority of avoidable adverse events are due to the lack of effective communication. Recent data suggests that standardization of the postoperative handoff process of children undergoing surgery improves outcomes.
(b)
Using the acronym SHARE, transitions can become more efficient, informative and safe.
(i)
Standardize critical content, including:
1.
Providing details of the infant’s history to the receiver.
2.
Emphasizing key information about the infant when speaking with the receiver.
3.
Synthesizing clinical information from separate sources before passing it on to the receiver.
(ii)
Hardwire within your system, including:
1.
Preparing and stating expectations about how to conduct a successful hand-off.
2.
Developing standardized forms, tools and methods, such as checklists.
3.
Using a quiet workspace or setting that is conducive to sharing information about a patient.
(iii)
Allow opportunities to ask questions, including:
1.
Using critical thinking skills and scrutinizing and questioning the data.
2.
Sharing and receiving information as an interdisciplinary team.
3.
Exchanging contact information in the event there are any additional questions.
(iv)
Reinforce quality and measurement, including:
1.
Demonstrating leadership commitment to successful hand-offs.
2.
Monitoring compliance with use of standardized forms, tools and methods for hand-offs.
3.
Using data to determine a systematic approach for improvement.
(v)
Get Clinical Tree app for offline access

Educate, including:
1.




Teaching staff and standardizing training on how to conduct a hand-off.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree