chapter 15 Musculoskeletal Examination
Normal Musculoskeletal Variants
Internal femoral torsion (femoral anteversion)
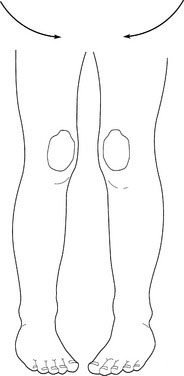
When children have internal femoral torsion, the patellas show internal strabismus (Fig. 15–1). Gently rotate the knees so that the patella face forward. If internal femoral torsion is the problem, the feet suddenly and miraculously point directly forward.
Bowleg (genu varum) and knock knees (genu valgum)
Mild lower extremity bowing is the norm in infants and young children (Fig. 15–2). Internal tibial torsion often accompanies physiologic bowing and accentuates the bowed appearance. No treatment is necessary. By age 2 years, physiologic bowing spontaneously corrects itself in most children. Many healthy children, including those who have had physiologic bowing as toddlers, gradually convert to develop some degree of genu valgum after age 2 years (Fig. 15–3), which usually disappears spontaneously by age 8 years.
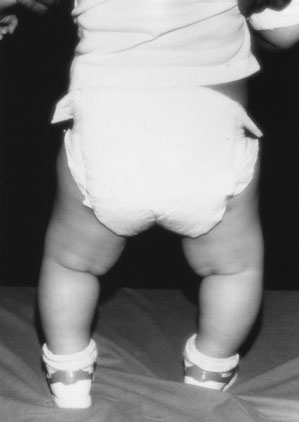
FIGURE 15–2 Genu varum (nonrachitic bowing of the legs), a transient normal variant requiring no treatment.

Metatarsus varus (forefoot adduction)
In metatarsus varus, the forefoot turns inward in relation to the long axis of the heel (Fig. 15–4). The critical clinical issue is to determine whether the foot deformity is fixed or flexible. Mild to moderate flexible metatarsus varus usually corrects itself, because it is the result of intrauterine position, or packing. A severe or fixed metatarsus varus may require serial casting or an orthotic device. If you are in doubt about the severity of this condition in a child, consult a pediatric orthopedist.

Flat feet
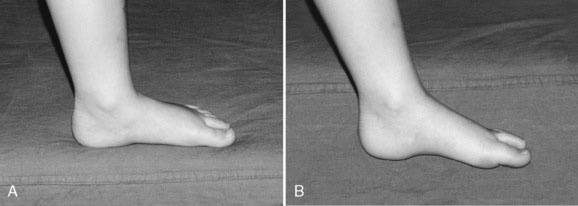
Flat feet are the norm in children younger than ages 2 to 3 years and in older children who show greater than average joint mobility. Usually asymptomatic, this normal variant is often simply part of generalized hypermobility. In such children, the normal body weight is sufficient to cause flattening of the feet. When the youngster sits on a table, the longitudinal arch miraculously reappears as the feet are suspended in space (Fig. 15–5).
Slipped Capital Femoral Epiphysis
Slipped capital femoral epiphysis occurs in adolescents. Presenting symptoms include:
Knee pain
Knee pain in children is often due to one of the following causes:
Back pain
Consider osteomyelitis of a vertebral body, discitis, or tumor in all children who present with back pain. Other causes are discussed here.
Generalized Causes of Musculoskeletal Pain
Tumors
Juvenile idiopathic arthritis
Arthritis is defined by the American College of Rheumatology as the presence of joint swelling or two or more of the following findings:
Benign hypermobility
Benign hypermobility syndrome is a common cause of joint pain, particularly in the knees, ankles, and fingers. Occasionally, the affected joints appear swollen for brief periods, but the swelling resolves spontaneously. The symptoms are episodic and may be exacerbated by exercise. The clinical findings that allow you to make a diagnosis of hypermobility are listed in Box 15–1.
The Child with a Limp
Causes of an abnormal gait may be divided into the following categories:
A limp is frequently accompanied by pain in a child, although discomfort may not be the chief complaint (Table 15–1). Recent pain accompanied by worsening symptoms suggests trauma, infection, slipped capital femoral epiphysis, or transient synovitis. The more prolonged the symptoms, the more likely that an abnormality will be detected on imaging studies. A limp that is worse in the morning and improves as the day progresses may be due to inflammatory disease. Limping without pain occurs in conditions such as developmental hip dysplasia, leg-length discrepancy, and neurological disorders.
TABLE 15–1 Common Causes of a Limp in a Child
| Cause | Underlying Conditions |
|---|---|
| Local causes | |
| Hip | Developmental hip dysplasia, |
| Legg-Calvé-Perthes disease (septic arthritis), transient synovitis, slipped capital femoral epiphysis | |
| Knee | Osgood-Schlatter disease, osteochondritis dissecans, tumors |
| Tibia | Toddler’s fracture, stress fracture, fracture through a bone cyst |
| Foot | Tarsal coalition, Köhler disease, tight shoes |
| Back | Spondylolisthesis, osteomyelitis, |
| Scheuermann disease | |
| Short leg | |
| Generalized disorders | |
|---|---|
| Bone diseases | Rickets, infections, leukemia, primary tumors |
| Muscle diseases | Inflammatory, congenital, metabolic myopathies |
| Joint diseases | Juvenile idiopathic arthritis, septic arthritis |
| Neurological diseases | Cerebral palsy |
| Psychiatric diseases | Conversion disorder |
The Child with a Single Swollen Joint
Six broad categories of monoarthritis are listed in Box 15–2. As with musculoskeletal pain, the location provides a diagnostic clue, particularly in rheumatic or orthopedic conditions.



