CHAPTER 17 MUSCLE AND NERVE PATHOLOGY
MUSCLE BIOPSY
Overview

• Due to their specialist nature, should only be reported by pathologists with a specialist interest in muscle disease and in department familiar with handling these samples




• Few diagnoses can be safely made on muscle biopsy in absence of good clinical information including








Specimen handling
• Muscle biopsies must be transported fresh to the laboratory rapidly wrapped in a damp piece of gauze



Histochemical and immunohistochemical stains














Myopathic changes
• For full discussion of interpretation of muscle biopsies reference should be made to specialist texts on muscle pathology
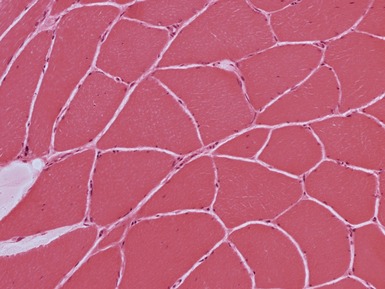
• General morphological changes that should be reported
 internal nuclei (Fig 17.1)
internal nuclei (Fig 17.1)
 internal nuclei (Fig 17.1)
internal nuclei (Fig 17.1)– geographically central nuclei (as opposed to simply internal) in centronuclear/myotubular myopathy









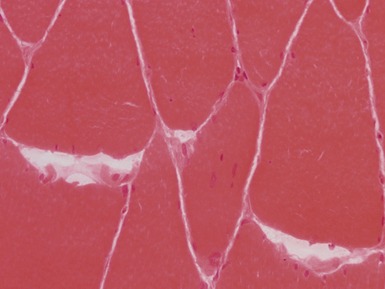
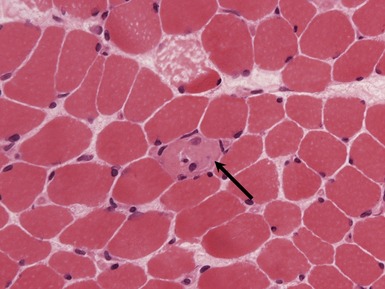
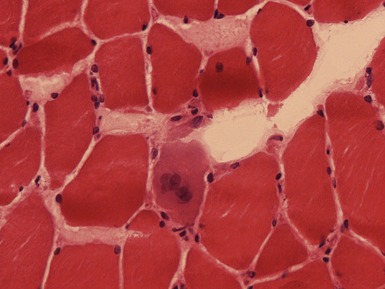
Fig 17.3 Photomicrograph showing a necrotic fiber (arrow). The fiber is pale and has been infiltrated by macrophages.





MUSCULAR DYSTROPHY





DYSTROPHINOPATHIES (DUCHENNE AND BECKER MUSCULAR DYSTROPHY)
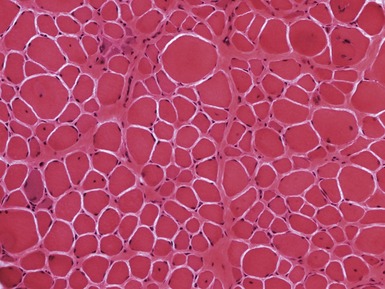
Fig 17.7 Photomicrograph of a muscle biopsy from a patient with Duchenne muscular dystrophy. There is marked variation in fiber size due to a mixture of atrophic and hypertrophic fibers. There are excess internal nuclei, increased endomysial collagen and regenerating fibers (see Fig 17.5 for detail).






Clinical features





Becker























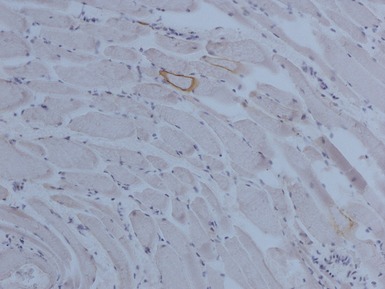
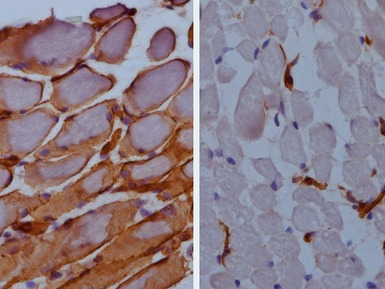
Immunohistochemical staining












FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY





DEFECTS IN NUCLEAR MEMBRANE PROTEINS (INCLUDING EMERY–DREIFUSS DYSTROPHY)


Clinical features








Limb girdle muscular dystrophy Type 1B (limb girdle muscular dystrophy with arterio-ventricular conduction block)










































LIMB GIRDLE MUSCULAR DYSTROPHIES (LGMD)
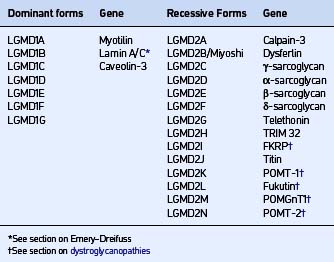
• Wide range of dystrophies associated with dominant (LGMD type 1) or recessive inheritance (LGMD type 2) (Guglieri et al 2008; Table 17.1)



CAVEOLINOPATHIES

















DYSFERLINOPATHIES





Immunohistochemical staining

SARCOGLYCANOPATHIES
• Mutations in one of four membrane proteins associated with the dystroglycan associated complex (Fig 17.11)
Genetics


Table 17.2 Sarcoglycanopathies
| Syndrome | Ethnicity | |
|---|---|---|
| α | LGMD2D | No association |
| β | LGMD2E | |
| γ | LGMD2C | |
| Severe childhood autosomal recessive muscular dystrophy (SCARMD) | North Africa | |
| Recessive muscular dystrophy of European Gypsies | European Gypsies | |
| δ | LGMD2F | Brazil |
Clinical features
• Clinically mimics dystrophinopathies from severe Duchenne-like presentation to asymptomatic hyperCKemia

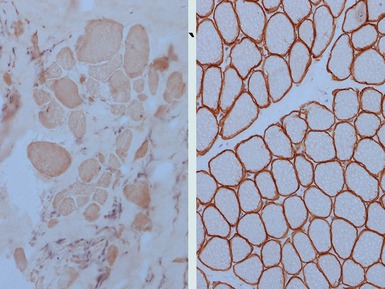
Immunohistochemical staining

• Complete loss of sarcoglycan staining with intact dystrophin is usually associated with sarcoglycan mutations







CONGENITAL MUSCULAR DYSTROPHIES

DYSTROGLYCANOPATHIES
• Diseases associated with deficiencies of O-linked glycosylation of α-dystroglycan (Muntoni et al 2008)




