Chapter 110 Menstrual Problems
Menstrual Irregularities
Menstrual cycle irregularities are described according to variation in frequency of menses, amount, and both frequency and amount (Table 110-1). Most menstrual cycle abnormalities are explained by maturation of the hypothalamic-pituitary-ovarian axis, although organic pathology should be considered and excluded in a logical and cost-effective manner. A complete history for evaluating a patient with menstrual dysfunction should include questions specifically related to puberty and menstrual patterns, a family history of gynecologic problems and maternal onset of menarche, and a medical history noting hospitalizations, chronic illness, medication or substance use, and infections. The related associations of weight change, nutrition, exercise, and sports participation can be critically important in considering a differential diagnosis. Regardless of the age of the adolescent, an appropriate history of any type of sexual activity should be elicited, and the pediatrician should be cognizant of the need to rule out sexual abuse as an issue in very young adolescents when other findings suggest sexual activity.
Table 110-1 TERMS FOR MENSTRUAL CYCLE IRREGULARITIES
VARIATIONS IN FREQUENCY
VARIATIONS IN AMOUNT
VARIATIONS IN AMOUNT AND DURATION
From Blythe MI: Common menstrual problems of adolescence, Adolesc Med 8:87–109, 1997.
Psychogenic factors have been implicated in amenorrhea. It is often difficult to separate psychologic from nutritional factors because weight loss is a common confounding variable in many of these situations, such as depression (Chapter 24), anorexia nervosa (Chapter 26), or stress.
110.1 Amenorrhea
Differential Diagnosis
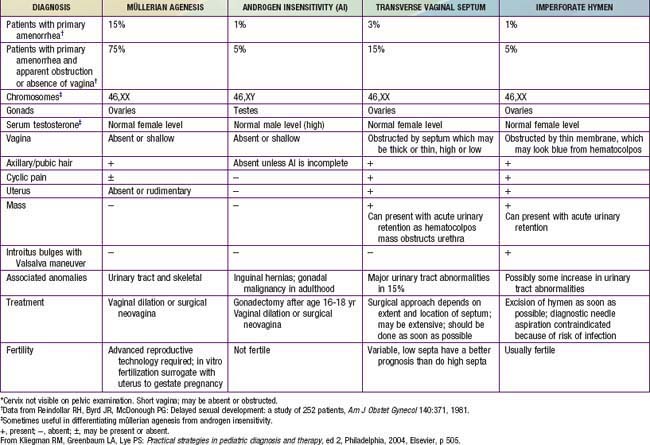
In primary amenorrhea, defined as failure for menstruation to begin, chromosomal or congenital abnormalities, such as gonadal dysgenesis, triple X syndrome, isochromosomal abnormalities, testicular feminization syndrome, and, rarely, true hermaphroditism, should be considered in addition to the conditions that cause secondary amenorrhea (Table 110-2). Elevated levels of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) suggest primary gonadal failure, and chromosome analysis often elucidates its cause. When primary amenorrhea occurs with otherwise normal progression of pubertal development, a structural anomaly of the müllerian duct system (Chapter 548) should be suspected. Imperforate hymen is most the common disorder of müllerian duct descent and is associated with recurrent (monthly) abdominal pain and, after some time has passed, a midline, lower abdominal mass, which is the blood-filled vagina, and is called hematocolpos. Diagnosis is made by inspection of the introitus, revealing a bulging hymen with bluish discoloration. If the obstruction is at the level of the cervix, the blood-filled uterus (hematometrium) is apparent on bimanual examination or ultrasonography. Agenesis of the cervix or uterus is rare but occurs in association with sacral agenesis.
Primary or secondary amenorrhea may also be caused by chronic illness, particularly that associated with malnutrition or tissue hypoxia, such as diabetes mellitus, inflammatory bowel disease, cystic fibrosis, or cyanotic congenital heart disease. In most cases, the illness has been diagnosed previously, but, occasionally, the amenorrhea is its first manifestation. Pregnancy is a common cause of secondary and occasionally primary amenorrhea. Polycystic ovarian syndrome (PCOS) (Chapter 580.2) is one of the most common endocrine disorders affecting 4-6% of premenopausal women and presents with menstrual abnormalities that range from amenorrhea to dysfunctional uterine bleeding. The criterion for the diagnosis of PCOS is menstrual irregularity in the face of androgen excess with either hirsutism, acne, or increased serum androgens. When the androgen excess is coupled with insulin resistance and acanthosis nigricans, the term HAIR-AN syndrome is used. A central nervous system (CNS) tumor, most commonly a craniopharyngioma, may present with amenorrhea. Prolactinomas, although rare, are the most common pituitary tumor in adolescence. Abnormalities of the thyroid gland, typically hyperthyroidism, may first be suspected by delayed sexual maturation or amenorrhea, even in the absence of other signs and symptoms. Hypothyroidism may cause precocious puberty but may also be associated with delayed puberty or abnormal uterine bleeding. Anorexia nervosa, which may present with either primary or secondary amenorrhea, is occasionally confused with hyperthyroidism because of weight loss, hyperactivity, and personality changes seen in both entities. Amenorrhea is one of the components of the female athlete triad in association with disordered eating and low bone mass (Chapter 682). Ballerinas, gymnasts, and runners may be at disproportionate risk of this triad. Ingestion of drugs, both legal and illegal, may cause amenorrhea and, in the case of phenothiazines, even a false-positive urine pregnancy test. Some drugs, including phenothiazines and certain antihypertensive agents, may cause galactorrhea, further mimicking pregnancy. Pertinent findings on physical exam include signs of androgen excess, such as obesity, acne, hirsutism, and clitoromegaly, along with excessive thinness, galactorrhea, and thyromegaly. Adolescents with amenorrhea who diet, whether or not they meet diagnostic criteria for anorexia nervosa, are at risk for low bone density.



